Abortion statistics, England and Wales: 2021
Updated 2 April 2024
Applies to England and Wales

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/statistics/abortion-statistics-for-england-and-wales-2021/abortion-statistics-england-and-wales-2021
Key events
| Date | Key event |
|---|---|
| October 1967 | Abortion Act 1967 passed. Introduced by David Steel and supported by the government under a free vote. It legalised abortion on certain grounds, by legalised practitioners, in England, Wales and Scotland. The act came into effect on 27 April 1968. |
| November 1990 | The Human Fertilisation and Embryology Bill lowered the gestation limit for abortions from 28 weeks to 24 weeks. This is the currently accepted point at which the fetus is considered viable outside the mother’s body. The act came into effect on 1 April 1991. |
| June 2017 | Northern Ireland funding scheme introduced, to provide funded abortions in England and Wales, for residents of Northern Ireland. In cases of hardship, travel costs are also covered. Funding is provided by the Government Equalities Office and HM Treasury. |
| June 2018 | Women in Wales, and from 28 December 2018 women in England, can take the second of the 2 abortion pills, misoprostol, at home. This brought England and Wales in line with Scotland, which allowed the second pill to be taken at home from October 2017. |
| December 2018 | Abortion legalised on certain grounds, in the Irish Republic, up to 12 weeks gestation and later if the woman’s life or health is at risk. The law came into effect on 20 December 2018. |
| October 2019 | Abortion in Northern Ireland decriminalised after a free vote by Westminster MPs in July 2019. The suspended Northern Ireland Executive did not return by 21 October 2019, meaning the amendment introduced by Stella Creasy was passed into law through The Northern Ireland (Executive Formation etc) Act 2019 on 22 October 2019. |
| March 2020 | Women in England and Wales can take both abortion medications, mifepristone and misoprostol, at home, without the need to first attend a hospital or clinic. This has been temporarily approved by the Secretary of State for Health and Social Care to limit the transmission of coronavirus (COVID-19) from 30 March 2020 and by the Welsh government’s Minister for Health and Social Services from 31 March 2020. |
| March 2020 | The Abortion (Northern Ireland) Regulations 2020 came into force on 31 March 2020. The regulations introduce a new legal framework for abortion services in Northern Ireland. |
| February 2022 | The temporary measures, put in place in March 2020 to allow women in Wales to take both abortion medications at home, were made permanent from 24 February 2022. |
| March 2022 | On 30 March 2022, Parliament voted in favour of an amendment to the Health and Care Bill, making the temporary approval allowing home use of both pills for early medical abortions permanent in England and Wales. These provisions will supersede the arrangements made permanent in Wales in February 2022. |
Key points in 2021
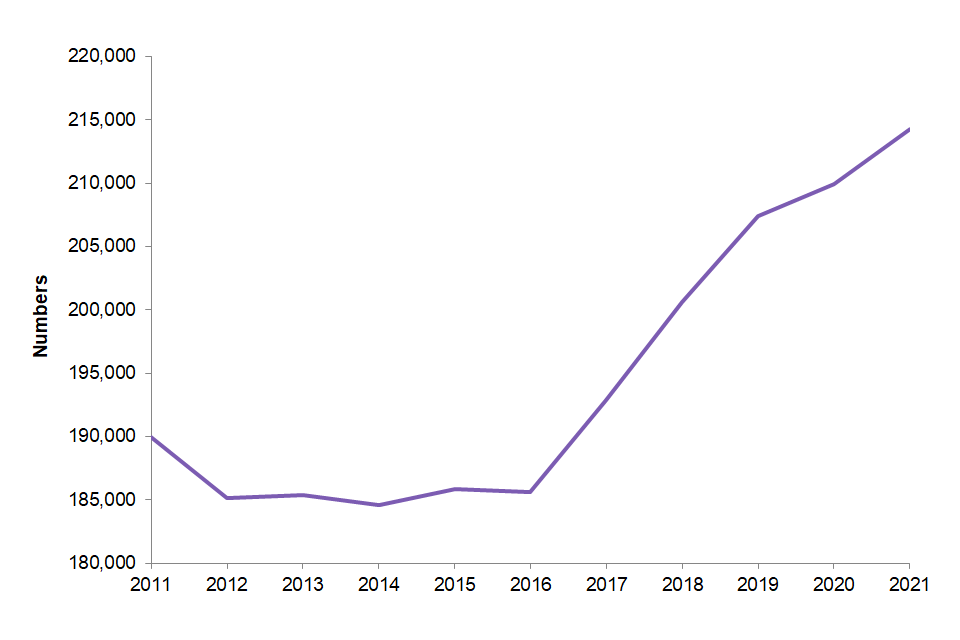
There were 214,256 abortions for women resident in England and Wales, the highest number since the Abortion Act was introduced.
Figure 1: number of abortions, England and Wales, 2011 to 2021
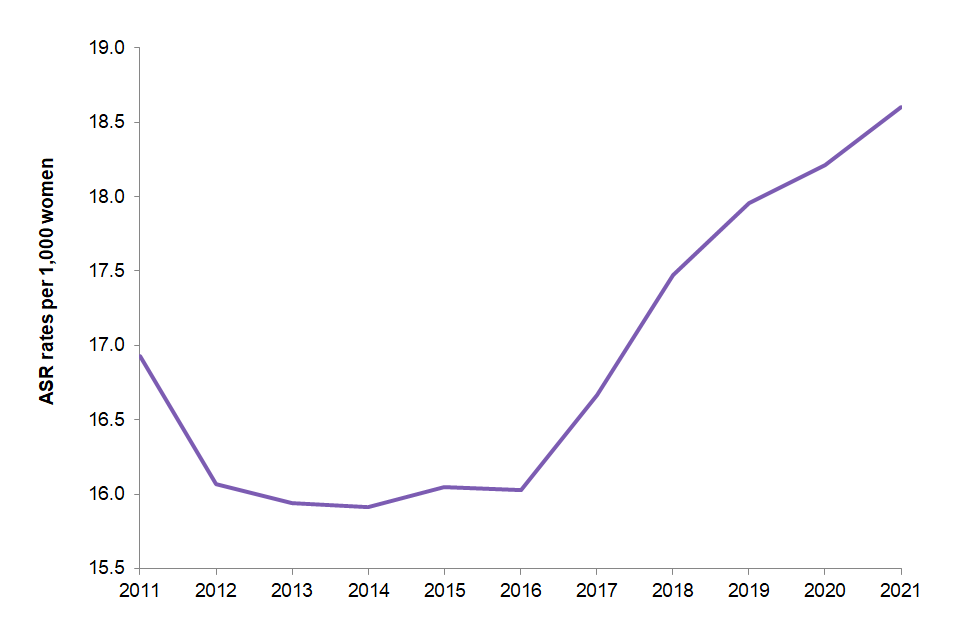
The age standardised abortion rate for residents is 18.6 per 1,000 women, the highest rate since the Abortion Act was introduced.
Figure 2: age standardised abortion rate, England and Wales, 2011 to 2021
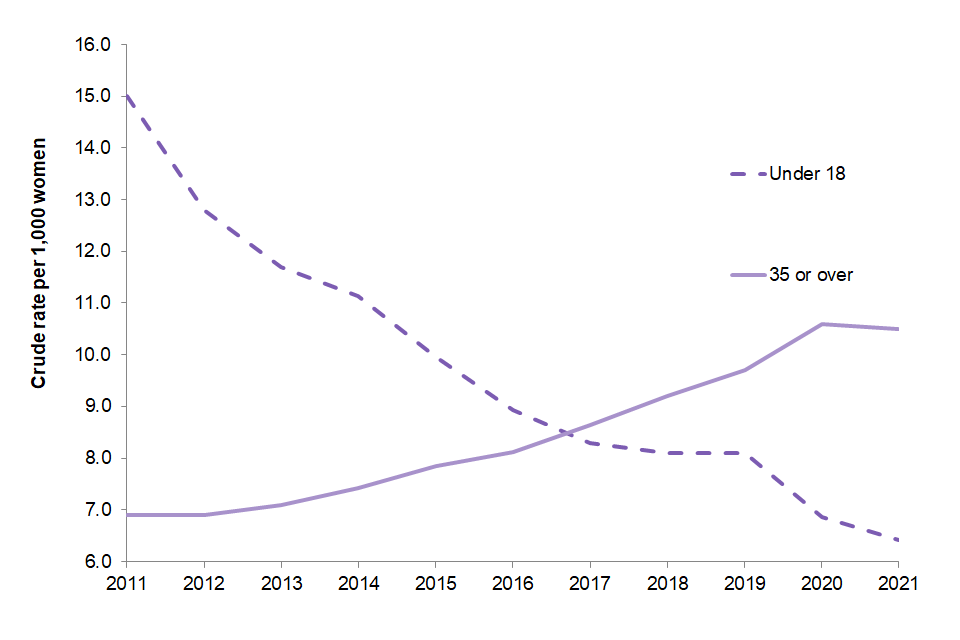
However, the abortion rate for women aged under 18 has continued to decrease (from 15.0 in 2011 to 6.9 in 2020 and further decreased to 6.4 per 1,000 in 2021). The rate has remained stable for women aged 35 or over (from 10.6 to 10.5 per 1,000 between 2020 and 2021).
Figure 3: crude abortion rates for under 18 and over 35, England and Wales, 2011 to 2021
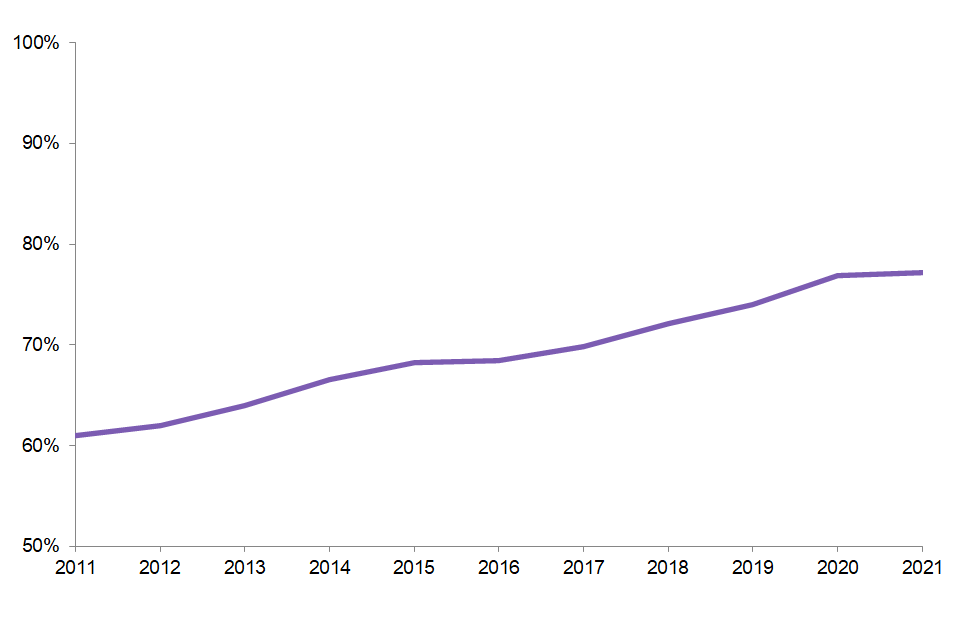
99% of abortions in England and Wales were funded by the NHS in 2021, with 77% of abortions taking place in the independent sector.
Figure 4: percentage of abortions that were NHS funded and performed in the independent sector, England and Wales, 2011 to 2021
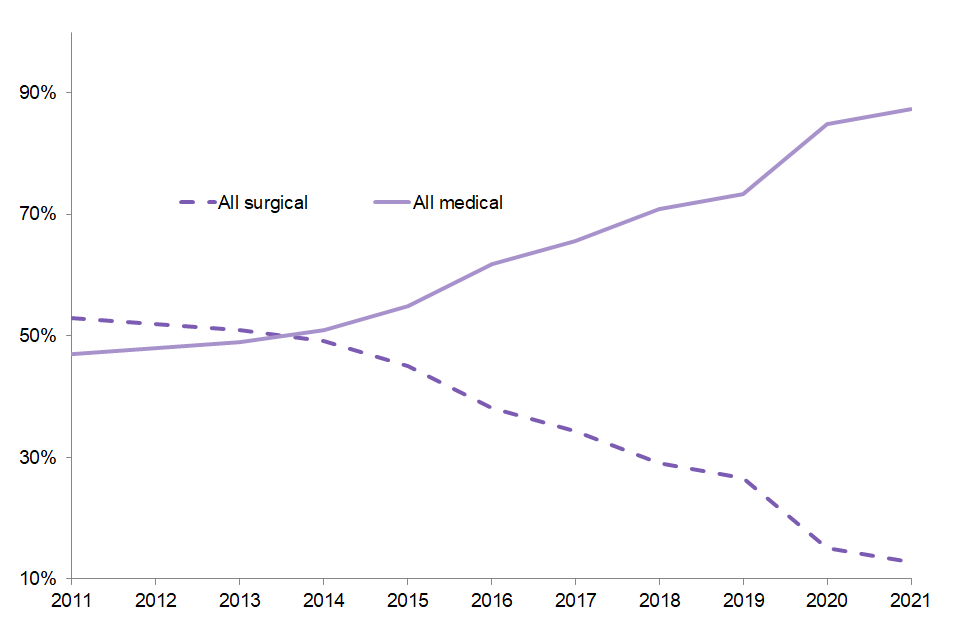
87% of abortions were medically induced, which increased from 85% in 2020. It has increased by 40 percentage points since 2011.
Figure 5: percentage of abortions by procedure type (medical or surgical), England and Wales, 2011 to 2021
Introduction
This report provides statistics on abortions recorded in England and Wales in 2021. The information presented is based on abortion notification forms (HSA4) submitted by clinics and hospitals to the Chief Medical Officer (CMO) at the Department of Health and Social Care (DHSC) together with forms submitted to the Welsh CMO. DHSC monitor the forms to ensure that there is full compliance with the legislation set out in the Abortion Act, 1967.
The COVID-19 pandemic has had an impact on numbers of abortions, and method of abortion. Further information is set out in the different sections below, where relevant.
Further information
Further details on the legislative context of the Abortion Act, in addition to methodological and technical information on the data can be found in the ‘Guide to Abortion Statistics’, in Abortion statistics for England and Wales: 2021.
Previous publications
The DHSC has published abortion statistics annually since 2002. Statistics for years from 1968 to 1993 were published by the Office of Population Censuses and Surveys, then their successor Office for National Statistics (ONS) from 1994 to 2001. Reports up to and including 2001 are available electronically on request to abortion.statistics@dhsc.gov.uk.
The most recent versions of the publication (2002 onwards) are available in the abortion statistics for England and Wales collection.
Abortion statistics cover the period January to December and are published annually. The next publication will be in June 2023, and will cover January to December 2022. For further information or to provide any feedback on the publication, contact us at abortion.statistics@dhsc.gov.uk.
Commentary
Unless specified, the following commentary, charts and tables relate only to abortions in England and Wales, for residents of England and Wales, in 2021.
Unless otherwise stated the rates presented in this publication are based off abortions per 1,000 women aged 15 to 44.
Overall number and rate of abortions
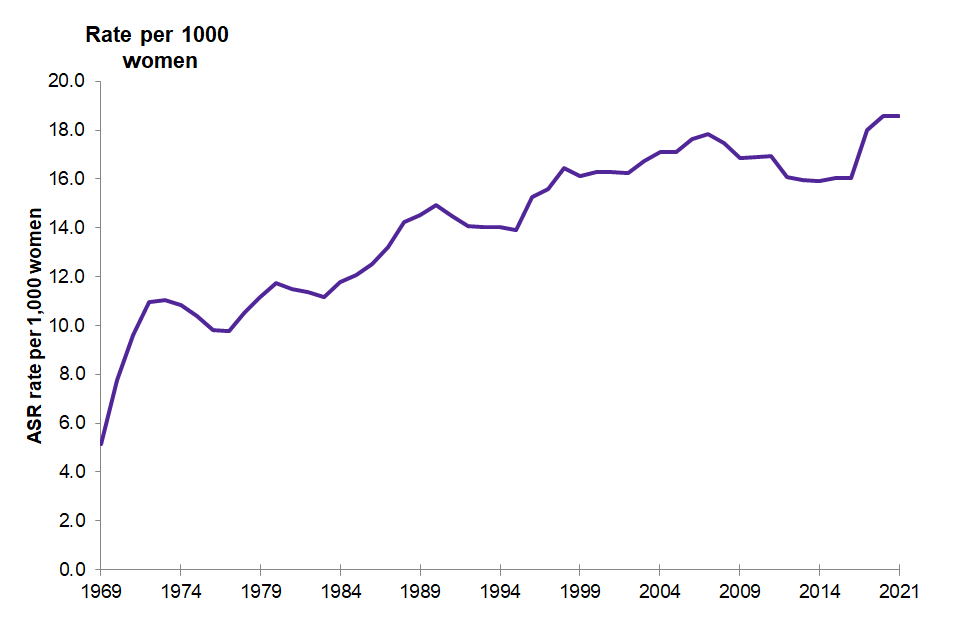
214,869 abortions were reported in England and Wales in 2021, the highest since records began. The vast majority of these abortions (214,256) were to residents of England and Wales. This represents an age-standardised abortion rate (ASR) of 18.6 per 1,000 resident women aged 15 to 44. This is the highest rate recorded, exceeding the previous peak in 2020, (18.2 abortions per 1,000 resident women aged 15 to 44). (Table 1 and Figure 6).
Figure 6: age standardised abortion rate per 1,000 women aged 15 to 44, England and Wales, 1969 to 2021
Age
The abortion rate in 2021 was highest for women aged 22 (at 31.0 per 1,000 women). In 2020 the highest rate was for women aged 21 (30.6 per 1,000 women), and in 2011 it was highest for women aged 20 (at 32.6 per 1,000 women).
Figure 7: crude abortion rate per 1,000 women by single year of age, England and Wales, 2011 and 2021
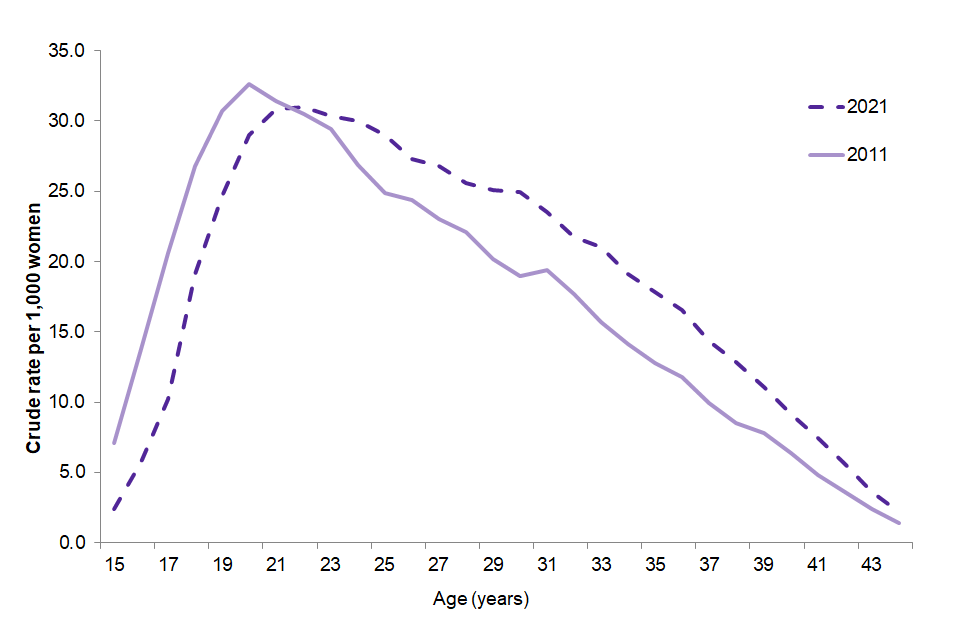
There has been an increase in the rates for all ages 22 and above over the last 10 years. The largest increases in abortion rates by age are among women aged 30 to 34 which have increased from 17.2 per 1,000 in 2011 to 22.1 per 1,000 in 2021.
Abortion rates for those aged under 18 have declined over the last 10 years (from 15.0 to 6.4 per 1,000 between 2011 and 2021). The decline since 2011 is particularly marked in the under 16 age group, where the rates have decreased from 3.4 per 1,000 women in 2011 to 1.1 per 1,000 women in 2021. The abortion rate for 18 to 19 year olds has also declined from 28.8 per 1,000 women to 22.0 per 1,000 women in the same period (Table 3b).
Marital status
82% of abortions in 2021 were for women whose marital status was given as single, a proportion that has remained roughly constant for the last 10 years. 49% were to women whose marital status was given as single with a partner. This proportion has remained similar in recent years (Table 3).
Ethnicity
Ethnicity was recorded on 91% of the forms received for 2021 (Table 3); this compares to 95% of forms received for 2020. Where ethnicity was recorded, 78% of women having abortions reported their ethnicity as White, 9% as Asian, 7% as Black, 5% as Mixed and 1% as Other.
Area of residence within England and Wales
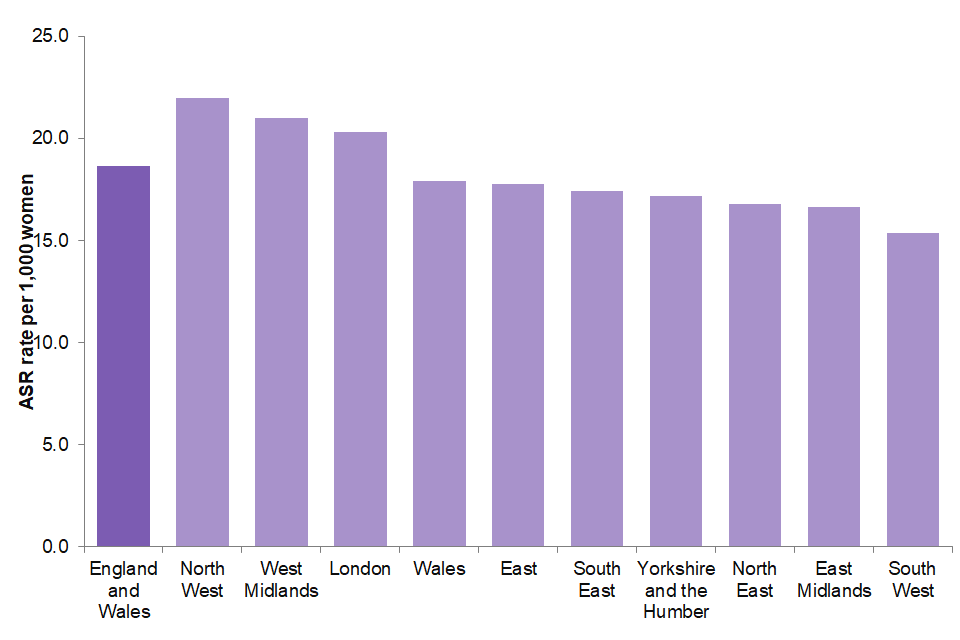
By region of residence, rates of abortion are highest in the North West (22.0 per 1,000 women aged 15 to 44) and lowest in the South West (15.4 per 1,000 women aged 15 to 44). (Figure 8).
Figure 8: age standardised abortion rate, per 1,000 women aged 15 to 44, by region in England and Wales, 2021
Location and funding of abortions
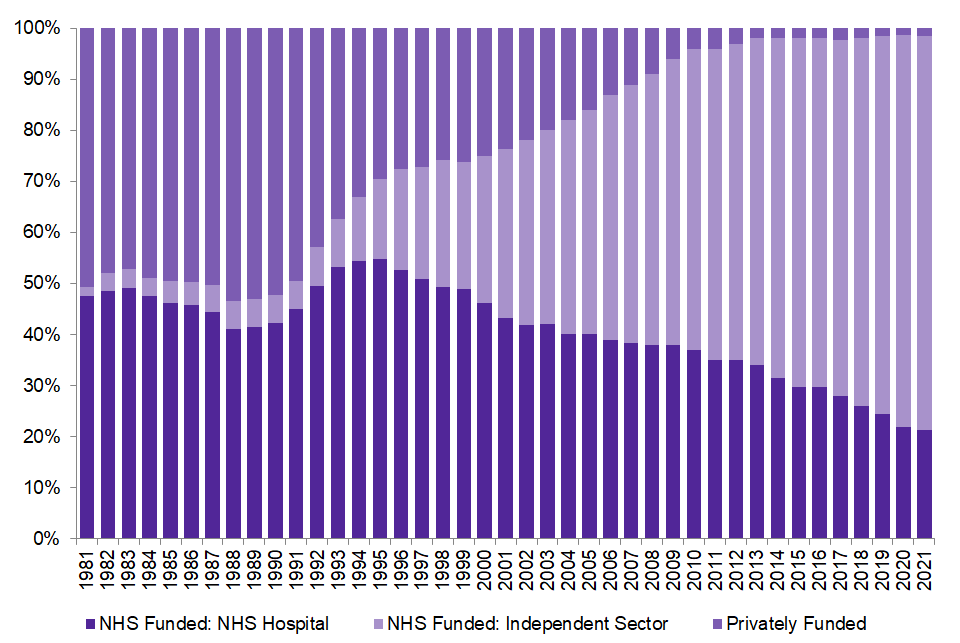
In 2021, 21% of abortions were performed in NHS hospitals. The percentage performed in approved independent sector clinics under NHS contract has remained consistent in 2020 and 2021, with these clinics performing 77% of abortions, making a total of 99% of abortions funded by the NHS. The remaining 1% were privately funded. (Table 3a.i and Figure 9).
The proportion performed in the independent sector under NHS contract has increased almost every year since this information was collected in 1981, while the proportions of NHS hospital and private abortions has fallen over this period.
Figure 9: percentage of abortions by purchaser/provider, England and Wales, 1981 to 2021
Statutory grounds for abortion
Under the Abortion Act 1967, a pregnancy may be lawfully terminated by a registered medical practitioner in approved premises, if 2 medical practitioners are of the opinion, formed in good faith, that the abortion is justified under one or more of grounds A to G. (Table A). For more information about the grounds for abortion, see the Glossary below and the guide to abortion statistics.
Table A: grounds for abortion
| Ground | Definition |
|---|---|
| Ground A | That the continuance of the pregnancy would involve risk to the life of the pregnant woman greater than if the pregnancy were terminated. |
| Ground B | That the termination is necessary to prevent grave permanent injury to the physical or mental health of the pregnant woman. |
| Ground C | That the pregnancy has NOT exceeded its 24th week and that the continuance of the pregnancy would involve risk, greater than if the pregnancy were terminated, of injury to the physical or mental health of the pregnant woman. |
| Ground D | That the pregnancy has NOT exceeded its 24th week and that the continuance of the pregnancy would involve risk, greater than if the pregnancy were terminated, of injury to the physical or mental health of any existing child(ren) of the family of the pregnant woman. |
| Ground E | That there is substantial risk that if the child were born it would suffer from such physical or mental abnormalities as to be seriously handicapped. |
| Ground F | To save the life of the pregnant woman. |
| Ground G | To prevent grave permanent injury to the physical or mental health of the pregnant woman. |
The proportion of abortions performed under different grounds has remained similar to previous years. In 2021, 98.0% of abortions (209,939) were performed under ground C. A further 1.6% were carried out under ground E (3,370 abortions), with 0.4% (836 abortions) under ground D. The remaining grounds account for very few abortions; 111 in total across grounds A, B, F and G. (Table 2).
The vast majority (99.9%) of abortions carried out under ground C alone were reported as being performed because of a risk to the woman’s mental health. These were classified as F99 (mental disorder, not otherwise specified) under the International Classification of Disease version 10 (ICD-10).
Legal abortions performed under ground E
Ground E abortions are those performed because of fetal abnormality at any gestation. There were 3,370 abortions performed under ground E in 2021. This is a slight increase since 2020, when there were 3,083 (1%, 287 abortions) abortions performed under ground E (Table 3a).
In 2021, 65% of ground E abortions were performed medically and 87% of all abortions were performed medically. This is in comparison to 2020 when 73% of ground E and 85% of all abortions were performed medically (Tables 9c and 7a).
There were 565 (16.8%) ground E abortions at 22 weeks and over and 274 (8.1%) ground E abortions at 24 weeks and over (Table 9b).
The age group with the highest proportion of abortions performed under ground E is 35 and over (3.4% of abortions for this age group were performed under ground E) (Table 2).
There was a total of 5,096 conditions mentioned on ground E forms in 2021. This is an increase from 4,495 in 2020. The medical diagnoses are coded to the International Classification of Diseases (ICD10). For more information on issues with the reporting of ground E abortions see the guide to abortion statistics in the link for Abortion statistics for England and Wales: 2021 (page 7).
Congenital malformations (see the Glossary below), were the most common medical condition mentioned on HSA4 forms, making up 54% of conditions mentioned. Chromosomal abnormalities counted for 29% of conditions mentioned (see Table 9a).
Gestation period
Figure 10: percentage of abortions by gestation, England and Wales, 2011 to 2021
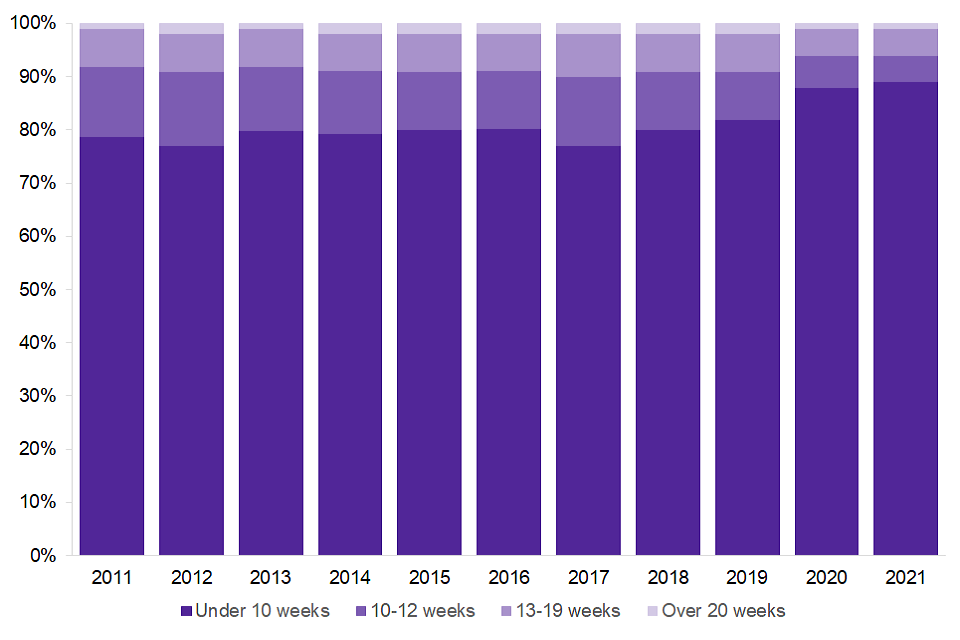
The proportion of abortions that are performed at under 10 weeks has continued to increase since 2011. In 2021, 89% of abortions were performed under 10 weeks, increasing from 88% in 2020 and 78% in 2011. The percentage performed at 20 weeks was 1% in both 2020 and 2021. (Table 3a.iii).
The legal limit for a woman having an abortion is 24 weeks gestation. This is the point at which the fetus is viable outside the mother’s body. Abortions may be performed after 24 weeks in certain circumstances, for example, if the mother’s life is at risk or the child would be born severely disabled. Abortions where gestation is 24 weeks or over account for a very small number of abortions (0.1% of the total). There were 276 such abortions in 2021. (Table 5).
Method of abortion
Different methods can be used to terminate a pregnancy, depending on the gestation, and other circumstances relating to the individual woman. There are medical methods which involve the use of drugs (for example, mifepristone) and there are surgical methods, such as vacuum aspiration or dilatation and evacuation. (See the Glossary below and guide to abortion statistics).
Figure 11: percentage of abortions by method, England and Wales, 2011 to 2021
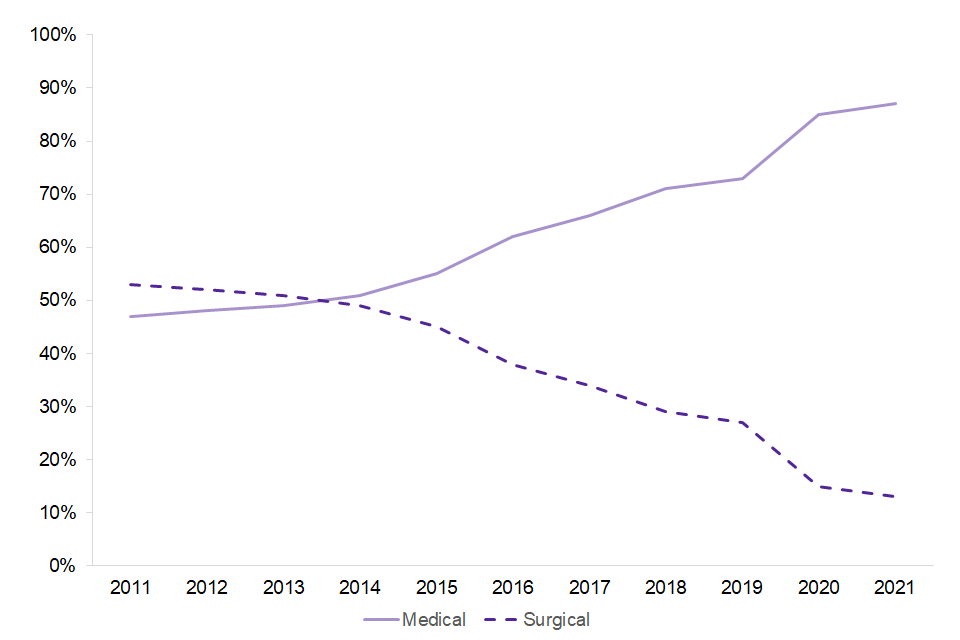
Medical abortions accounted for 87% of total abortions in 2021, an increase of 2 percentage points from 2020. There has been a continuing upward trend in medical abortions since 1991, when mifepristone was first licensed for use in the UK. (Table 3a.iv). There has been an additional effect during 2020 and 2021 due to the COVID-19 pandemic – more information on this is set out later in this commentary.
Early medical abortions are defined as taking place within the first 10 weeks of the pregnancy using medical methods. Until late March 2020, the first stage of treatment had to be administered at an NHS hospital or independent sector abortion clinic approved by the Secretary of State for Health and Social Care. Since June 2018 for Wales and December 2018 for England, women have been allowed to administer the second stage of treatment for early medical abortions at home.
From 30 March 2020, the Secretary of State for Health and Social Care approved temporary measures in England to limit the transmission of COVID-19 by approving the use of both pills for early medical abortion at home, without the need to first attend a hospital or clinic. Similar measures were put in place by the Welsh government’s Minister for Health and Social Services on 31 March 2020. These temporary measures remained in place throughout 2020 and 2021.
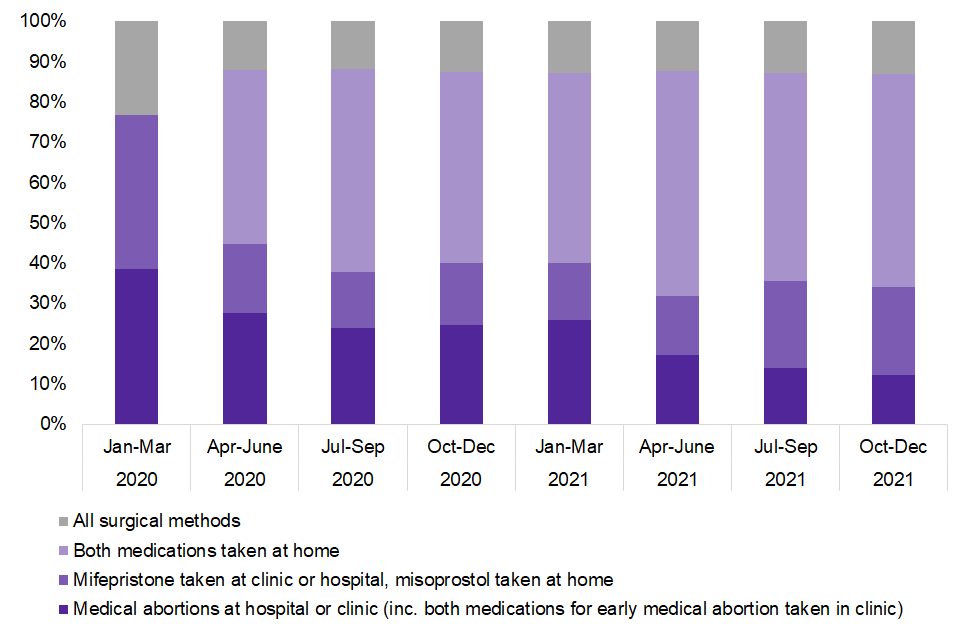
The percentages of different methods used to administer abortions have changed since the temporary approval of both pills for early medical abortion without needing to first visit a hospital or clinic (although it is worth noting the general increase in medical abortions over time). Taking both medications at home is the most common procedure, accounting for 52% of all abortions in 2021. Medical abortion overall accounted for 87% of abortions in 2021, compared to 88% of abortions for the last three quarters (April to December) of 2020. Medical abortions where mifepristone is taken in clinic and misoprostol is taken at home increased from 14% of abortions in the first quarter (January to March) of 2021 to 22% of abortions in the last quarter (October to December) of 2021. Taking both mifepristone and misoprostol at a hospital or clinic has become a less common method of abortion, decreasing from 37% of abortions in the first quarter (January to March) of 2020 to 24% in the fourth quarter (October to December) of 2020. This trend has continued in 2021, where taking both mifepristone and misoprostol at a hospital or clinic decreased from 25% of abortions in the first quarter (January to March) of 2021 to 12% in the fourth quarter (October to December) of 2021.
Figure 12: percentage of abortions performed by method, residents of England and Wales, quarterly, 2020 and 2021
For abortions at 22 weeks and over, feticide is recommended by the Royal College of Obstetricians and Gynaecologists, prior to the evacuation of the uterus, to stop the fetal heart. In 2021, of the 1,330 abortions performed at 22 weeks and over, 63% were reported as preceded by a feticide and a further 34% were performed by a method whereby the fetal heart is stopped as part of the procedure.
Previous abortions
In 2021, 43% of women undergoing abortions had had one or more previous abortions. The proportion has increased steadily from 36% in 2011 (Table 3a.ix and Table 4b).
The percentage of women aged under 18 who had one or more previous abortions has remained consistent at 7% in both 2011 and 2021. The percentage of women aged 30 or over, who had one or more previous abortions has increased from 46% in 2011 to 51% in 2021 (Table 4b).
There is large variation in rates of repeat abortions across local authorities. The proportion of women who had a repeat abortion in 2021 ranged from 29% (City of London) to 54% (Knowsley). This variation could be due to a range of factors, including random variation, differing demographics or the impact of local policy decisions. See Tables 10 and 11 for a wide range of additional analysis at local authority and clinical commissioning group (CCG) level.
Previous obstetric history
In 2021, 57% of women undergoing abortions had had one or more previous pregnancies that resulted in a live or stillbirth, up from 51% in 2011 (Table 3a.vii). 22% of women had a previous pregnancy resulting in a miscarriage or ectopic pregnancy, up from 17% in 2011.
Complications
Note that some of the figures quoted in this section were revised on 24 March 2023. See the ‘Revisions’ tab in the attachment Abortion statistics 2021: data tables (revision) for more information.
Data on complications should be treated with caution. It is not possible to fully verify complications recorded on HSA4 forms and complications that occur after discharge may not always be recorded. This means that for medical terminations where either both or the second stage was administered at home, complications may be less likely to be recorded on the HSA4. The Office for Health Improvement and Disparities (OHID) is currently undertaking a project to review the system of recording abortion complications data to address this going forward.
Complications were reported in 299 out of 214,256 cases in 2021; a rate of 1 in every 716 abortions (1.4 per 1,000 abortions), which is an increase from 2020 (1.2 per 1,000), and 2011 (1.0 per 1,000). The rate of surgical complications increased from 1.9 in 2020 to 3.8 in 2021. Medical complication rates for 2021 are similar to 2020; 1.6 in 2019 decreasing to 1.1 in 2020 and 1.0 in 2021. The decrease in the medical abortion complication rate between 2019 to 2021 coincides with the uptake of both medications at home. Due to how complications are recorded, for terminations where either both or the second stage is administered at home, complications may be less likely to be recorded. See the guide to abortion statistics for more information on reporting abortion complications (Table 8).
Selective terminations
In 2021, there were 88 abortions which were selective terminations (see Glossary below), an increase from 65 in 2020. 80% of the selective terminations were performed under ground E.
Women resident outside England and Wales
This section covers abortions carried out in England and Wales for women who are residents of other countries.
In 2021, there were 613 abortions to women recorded as residing outside England and Wales, a decrease from 943 in 2020. Most non-residents came from Northern Ireland (26.3%) and the Irish Republic (33.6%). The large decrease in the number of abortions for residents outside of England and Wales may be explained by travel restrictions in place throughout 2021 due to the COVID-19 pandemic and fewer women travelling from both Northern Ireland and the Irish Republic due to access and legislative changes in their respective countries (Table 12a).
Abortions for women from Northern Ireland
On 29 June 2017 the government announced that it would fund, via the Government Equalities Office (GEO), abortions for women ordinarily resident in Northern Ireland, where abortions were only available in very limited circumstances.
This provision for Northern Irish women currently remains in place despite the decriminalisation of abortion in Northern Ireland. On 19 May 2022, the Abortion (Northern Ireland) Regulations 2022 were laid, which removed barriers to commissioning abortion services. If the Northern Ireland Department of Health does not commission and fund abortion services, the regulations give the UK government power to do anything that a Northern Ireland minister or department could do for the purpose of ensuring that abortion services are provided.
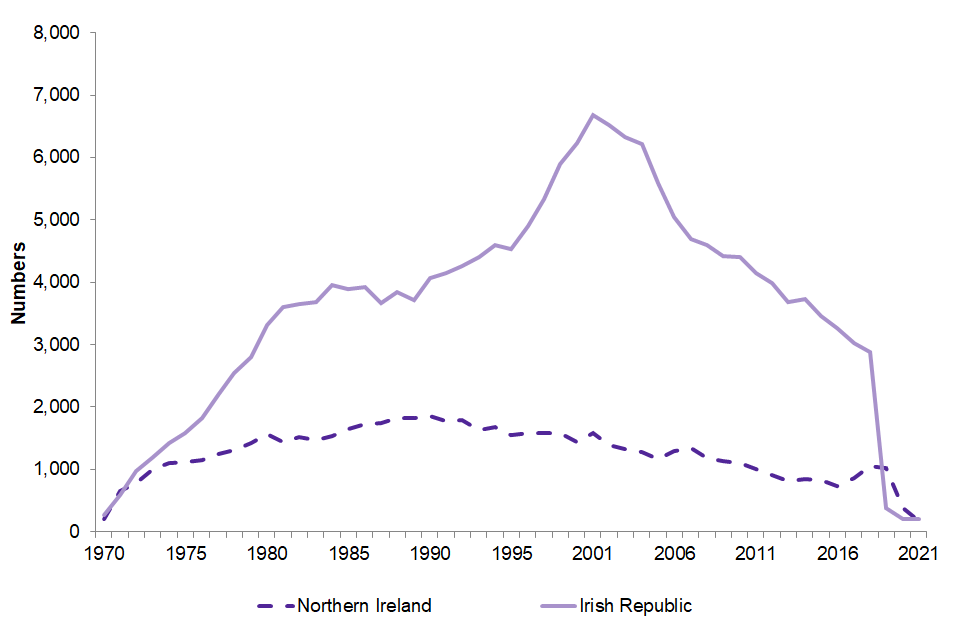
In 2021 there were 161 abortions for women from Northern Ireland, a significant decrease from the 371 in 2020. Current levels remain substantially lower than the peak of 1,855 Northern Ireland resident abortions in 1990.
Abortions for women from the Irish Republic
In May 2018 the ban on abortion in the Irish Republic was overturned, repealing the eighth amendment of the constitution. The law came into effect on 20 December 2018 meaning that abortion is permitted in the first 12 weeks of pregnancy and in later cases where the woman’s life or health is at risk, or in cases of fatal fetal abnormality.
As a result of this change and travel restrictions during the COVID-19 pandemic, in 2021, the number of women travelling to England and Wales for abortions declined from 2,879 in 2018 to 206 in 2021 (Table 12a), a decrease of 93%.
The proportion of abortions for residents of the Irish Republic performed under ground C was 50%, a decrease of 18 percentage points from 68% in 2020. The proportion of abortions performed under ground E increased from 32% in 2020 to 50% in 2021 (Table 12e). In 2021, 3.4% of abortions were performed at less than 10 weeks gestation, decreasing from 6.2% in 2020.
Figure 13: number of abortions for residents of Northern Ireland and the Irish Republic: 1970 to 2021
Abortion rates by Index of Multiple Deprivation (IMD), deciles
The Index of Multiple Deprivation (IMD) is the single official measure of relative deprivation available for England and Wales and provides the most effective way of understanding the differences in levels of deprivation between areas. Note that the Welsh and England IMD methodology differ, and their deciles are not comparable. The English IMD is based on deprivation across seven weighted domains (or types) of deprivation, while the Welsh IMD is based on deprivation across 8 weighted domains of deprivation, which combine to create the IMD by ranking each small area from most deprived to least deprived, typically dividing areas into 10 equal groups (or 10 deprivation deciles). Decile 1 is the most deprived and decile 10 the least deprived. For further information about the indices see the English Index of Multiple Deprivation 2019 and Welsh Index of Multiple Deprivation 2019.
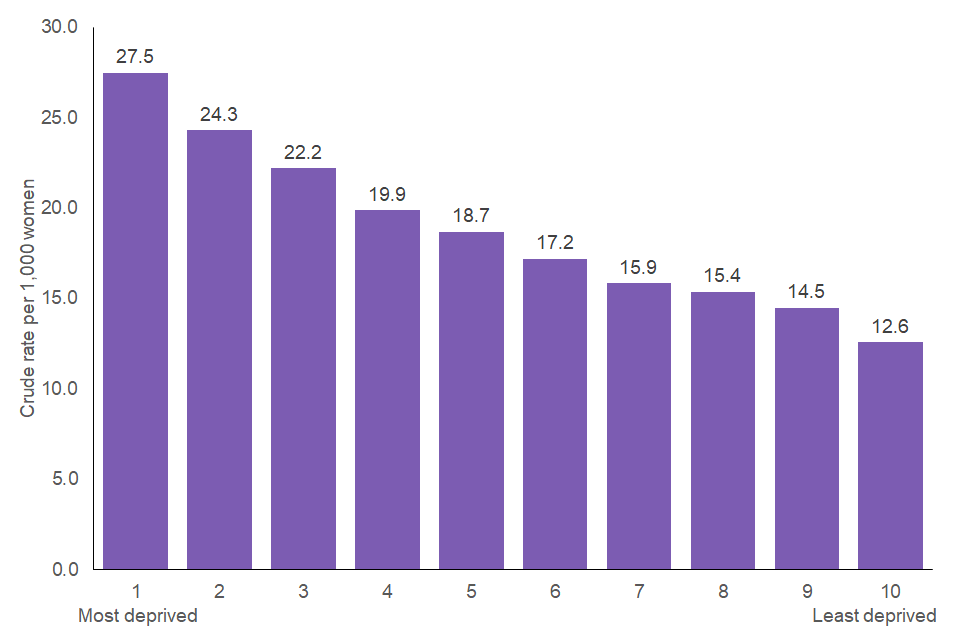
Women living in the most deprived areas of England are more than twice as likely to have abortions than women living in the least deprived areas. The rate in the most deprived decile is 27.5 per 1,000 women, compared to 12.6 per 1,000 women for women living in the least deprived areas. (Figure 14).
This is true across different age groups and different regions of England (Table 14 and Figure 14).
Figure 14: crude abortion rate per 1,000 women by IMD decile, England, 2021
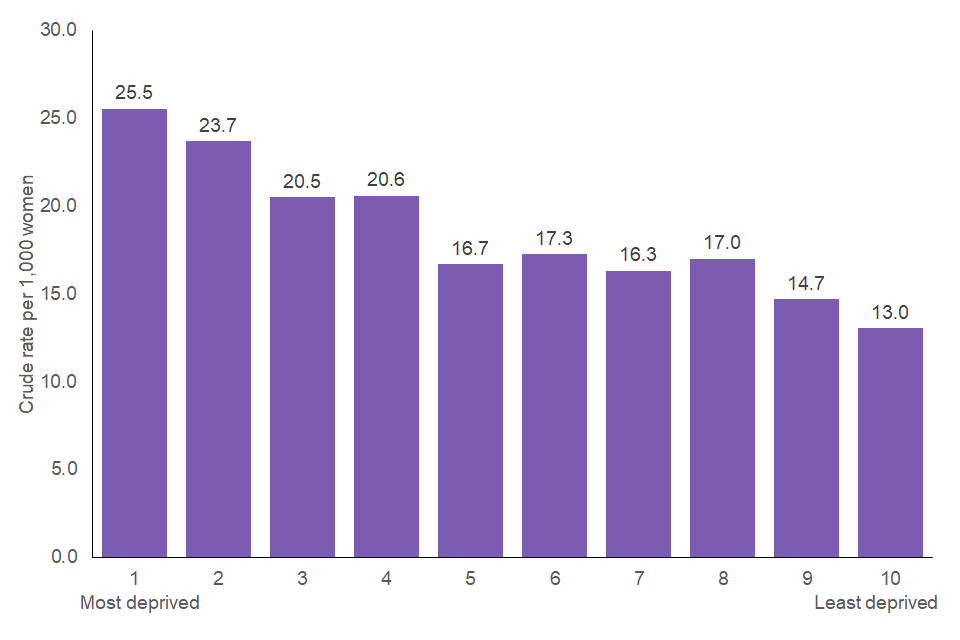
In Wales, women living in the most deprived areas are almost twice as likely to have abortions than women living in the least deprived areas. The rate in the most deprived decile is 25.5 per 1,000 women, compared to 13.0 per 1,000 women living in the least deprived areas. (Figure 15)
Figure 15: crude abortion rate per 1,000 women by IMD decile, Wales, 2021
Age range analysis by Index of Multiple Deprivation (IMD), deciles
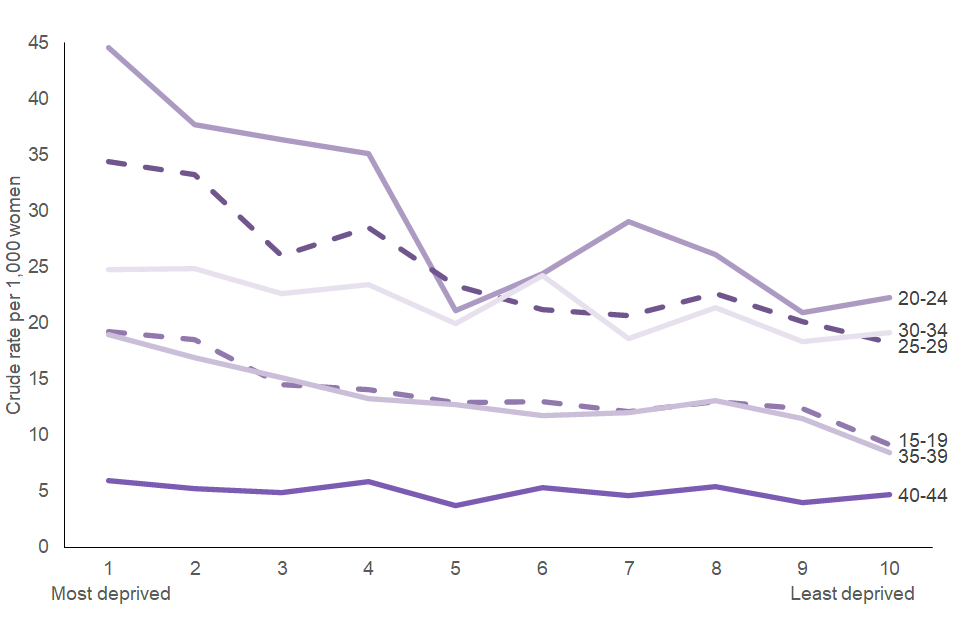
The trend of rates increasing as levels of deprivation increase is also consistent across all age ranges in both England and Wales (Figure 16 and 17).
Figure 16: crude abortion rate per 1,000 women, by age and IMD decile, England, 2021
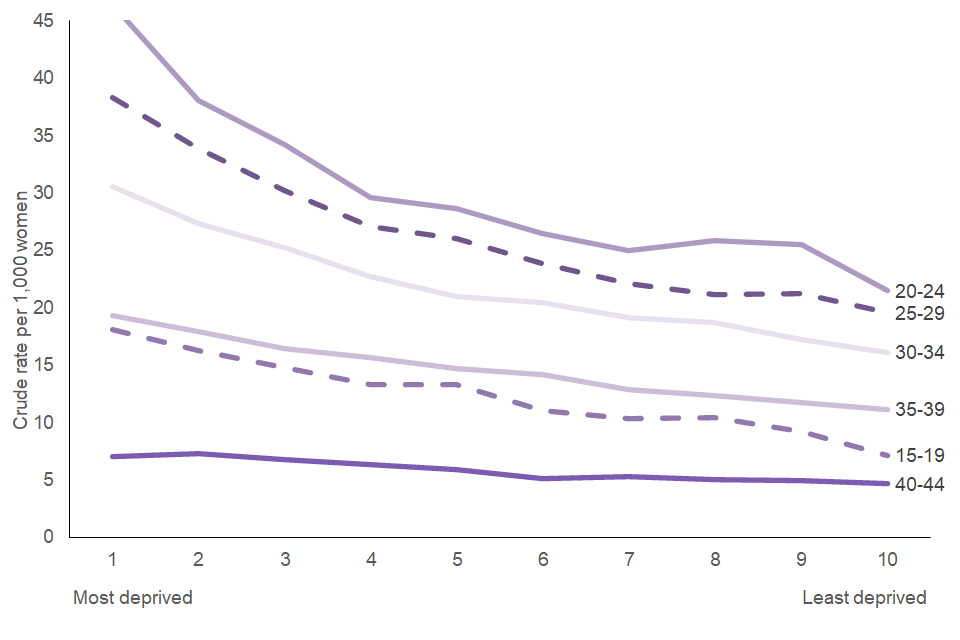
Figure 17: crude abortion rate per 1,000 women, by age and IMD decile, Wales, 2021
Glossary
Age standardised rate
A method to standardise the comparison of rates within populations where there are structural differences in age. (See the guide to abortion statistics for further details.)
Chief Medical Officer (CMO)
The CMO is the most senior government advisor on health matters in the UK. The CMO advises government on public health issues. This extends to recommending policy changes affecting the law governing abortion and advising doctors who perform abortions, regarding the interpretation of that law. There are 4 in total, each one advising either Her Majesty’s Government (CMO for England and medical adviser to the United Kingdom government), the Northern Ireland Executive, the Scottish government or the Welsh government.
Congenital malformation
Congenital malformations are also known as birth defects, congenital disorders or congenital anomalies. They are separated into 2 main types: structural disorders, which affect the shape of a body part and functional disorders, which affect how a body part works. Congenital malformations may include both structural and functional disorders.
Crude rate
The number of abortions in a specified population per year, divided by the total number of women in that population.
Grounds
The grounds for abortion are specified in Table A above and in the Abortion Act 1967.
Feticide
An abortion is a procedure to end a pregnancy. Feticide is the destruction of a fetus in the uterus.
Medical abortion
Two medicines are taken, the first is mifepristone and is taken at the clinic. The second is misoprostol, which may be taken at the same time or within 3 days of the first medicine. It may be taken either at the clinic or at home under amendments to the Abortion Act. From 30 March 2020 for England and the 31 March 2020 for Wales, temporary measures have been put in place to limit the transmission of COVID-19 by approving the use of both pills for early medical abortion at home, without the need to first attend a hospital or clinic. These were made permanent in Wales from 24 February 2022. On 30 March 2022, Parliament voted in favour of an amendment to the Health and Care Bill, making the temporary approval allowing home use of both pills for early medical abortions permanent in England and Wales.
Selective terminations
Pregnancies may result in more than one embryo being implanted in the womb. In such cases, the outcome of the pregnancy may be more successful if the number of fetuses is reduced. This reduction usually occurs at about 12 weeks gestation and is referred to as selective termination.
Surgical abortion
The pregnancy is removed in an operation by a doctor. There are 2 types. Vacuum aspiration is used between 3 and 12 weeks, where the fetus is removed by suction. Dilatation and evacuation is used between 13 and 24 weeks, where the fetus is removed using forceps.