
Lesion-Function Analysis from Multimodal Imaging and Normative Brain Atlases for Prediction of Cognitive Deficits in Glioma Patients

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. FET-PET and MR Imaging
2.3. MRI and FET-PET Image Segmentation
2.4. Determination of Lesion-Specific Damage to Functional Cortical Regions and White Matter Tracts
2.5. Cognitive Assessment
2.6. Statistical Analysis and Prediction of Cognitive Impairment
3. Results
3.1. Cognitive Test Scores in WHO Grade III/IV Glioma Patients
3.2. Impact of Total Lesion Volumes and Node or Tract Affection on Cognitive Function
3.3. Prediction of Cognitive Impairment
4. Discussion
4.1. Main Findings
4.2. Treatment-Related Tissue Damage and Recurrent Tumors as Causes for Cognitive Deficits
4.3. Impact of Lesion Location on Cognitive Deficits
4.4. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Kazmi, F.; Soon, Y.Y.; Leong, Y.H.; Koh, W.Y.; Vellayappan, B. Re-irradiation for recurrent glioblastoma (GBM): A systematic review and meta-analysis. J. Neurooncol. 2019, 142, 79–90. [Google Scholar] [CrossRef]
- Salvati, M.; Pesce, A.; Palmieri, M.; Floriana Brunetto, G.M.; Santoro, A.; Frati, A. The Role and Real Effect of an Iterative Surgical Approach for the Management of Recurrent High-Grade Glioma: An Observational Analytic Cohort Study. World Neurosurg. 2019, 124, e480–e488. [Google Scholar] [CrossRef]
- Weller, M.; van den Bent, M.; Tonn, J.C.; Stupp, R.; Preusser, M.; Cohen-Jonathan-Moyal, E.; Henriksson, R.; Le Rhun, E.; Balana, C.; Chinot, O.; et al. European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas. Lancet Oncol. 2017, 18, e315–e329. [Google Scholar] [CrossRef] [Green Version]
- Greene-Schloesser, D.; Robbins, M.E.; Peiffer, A.M.; Shaw, E.G.; Wheeler, K.T.; Chan, M.D. Radiation-induced brain injury: A review. Front. Oncol. 2012, 2, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pendergrass, J.C.; Targum, S.D.; Harrison, J.E. Cognitive Impairment Associated with Cancer: A Brief Review. Innov. Clin. Neurosci. 2018, 15, 36–44. [Google Scholar] [PubMed]
- Hirsch, J.; Ruge, M.I.; Kim, K.H.; Correa, D.D.; Victor, J.D.; Relkin, N.R.; Labar, D.R.; Krol, G.; Bilsky, M.H.; Souweidane, M.M.; et al. An integrated functional magnetic resonance imaging procedure for preoperative mapping of cortical areas associated with tactile, motor, language, and visual functions. Neurosurgery 2000, 47, 711–721. [Google Scholar]
- Satoer, D.; Vincent, A.; Ruhaak, L.; Smits, M.; Dirven, C.; Visch-Brink, E. Spontaneous speech in patients with gliomas in eloquent areas: Evaluation until 1 year after surgery. Clin. Neurol. Neurosurg. 2018, 167, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Satoer, D.; Vork, J.; Visch-Brink, E.; Smits, M.; Dirven, C.; Vincent, A. Cognitive functioning early after surgery of gliomas in eloquent areas. J. Neurosurg. 2012, 117, 831–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dallabona, M.; Sarubbo, S.; Merler, S.; Corsini, F.; Pulcrano, G.; Rozzanigo, U.; Barbareschi, M.; Chioffi, F. Impact of mass effect, tumor location, age, and surgery on the cognitive outcome of patients with high-grade gliomas: A longitudinal study. Neurooncol. Pract. 2017, 4, 229–240. [Google Scholar] [CrossRef]
- Hendriks, E.J.; Habets, E.J.J.; Taphoorn, M.J.B.; Douw, L.; Zwinderman, A.H.; Vandertop, W.P.; Barkhof, F.; Klein, M.; De Witt Hamer, P.C. Linking late cognitive outcome with glioma surgery location using resection cavity maps. Hum. Brain Mapp. 2018, 39, 2064–2074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satoer, D.; Visch-Brink, E.; Smits, M.; Kloet, A.; Looman, C.; Dirven, C.; Vincent, A. Long-term evaluation of cognition after glioma surgery in eloquent areas. J. Neurooncol. 2014, 116, 153–160. [Google Scholar] [CrossRef]
- van Kessel, E.; Snijders, T.J.; Baumfalk, A.E.; Ruis, C.; van Baarsen, K.M.; Broekman, M.L.; van Zandvoort, M.J.E.; Robe, P.A. Neurocognitive changes after awake surgery in glioma patients: A retrospective cohort study. J. Neurooncol. 2019, 146, 97–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosma, I.; Vos, M.J.; Heimans, J.J.; Taphoorn, M.J.; Aaronson, N.K.; Postma, T.J.; van der Ploeg, H.M.; Muller, M.; Vandertop, W.P.; Slotman, B.J.; et al. The course of neurocognitive functioning in high-grade glioma patients. Neuro-Oncol. 2007, 9, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Chapman, C.H.; Zhu, T.; Nazem-Zadeh, M.; Tao, Y.; Buchtel, H.A.; Tsien, C.I.; Lawrence, T.S.; Cao, Y. Diffusion tensor imaging predicts cognitive function change following partial brain radiotherapy for low-grade and benign tumors. Radiother. Oncol. 2016, 120, 234–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douw, L.; Klein, M.; Fagel, S.S.; van den Heuvel, J.; Taphoorn, M.J.; Aaronson, N.K.; Postma, T.J.; Vandertop, W.P.; Mooij, J.J.; Boerman, R.H.; et al. Cognitive and radiological effects of radiotherapy in patients with low-grade glioma: Long-term follow-up. Lancet Neurol. 2009, 8, 810–818. [Google Scholar] [CrossRef]
- Medaglia, J.D.; Lynall, M.E.; Bassett, D.S. Cognitive network neuroscience. J. Cogn. Neurosci. 2015, 27, 1471–1491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, A.; Kong, R.; Gordon, E.M.; Laumann, T.O.; Zuo, X.N.; Holmes, A.J.; Eickhoff, S.B.; Yeo, B.T.T. Local-Global Parcellation of the Human Cerebral Cortex from Intrinsic Functional Connectivity MRI. Cereb. Cortex 2018, 28, 3095–3114. [Google Scholar] [CrossRef] [PubMed]
- Yeo, B.T.; Krienen, F.M.; Sepulcre, J.; Sabuncu, M.R.; Lashkari, D.; Hollinshead, M.; Roffman, J.L.; Smoller, J.W.; Zollei, L.; Polimeni, J.R.; et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol. 2011, 106, 1125–1165. [Google Scholar] [PubMed]
- Mori, S.; Oishi, K.; Jiang, H.; Jiang, L.; Li, X.; Akhter, K.; Hua, K.; Faria, A.V.; Mahmood, A.; Woods, R.; et al. Stereotaxic white matter atlas based on diffusion tensor imaging in an ICBM template. Neuroimage 2008, 40, 570–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.A.; Petersen, J.; Maier-Hein, K.H. nnU-Net: A self-configuring method for deep learning-based biomedical image segmentation. Nat. Methods 2021, 18, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Boes, A.D.; Prasad, S.; Liu, H.; Liu, Q.; Pascual-Leone, A.; Caviness, V.S., Jr.; Fox, M.D. Network localization of neurological symptoms from focal brain lesions. Brain 2015, 138 Pt 10, 3061–3075. [Google Scholar] [CrossRef]
- Salvalaggio, A.; De Filippo De Grazia, M.; Zorzi, M.; Thiebaut de Schotten, M.; Corbetta, M. Post-stroke deficit prediction from lesion and indirect structural and functional disconnection. Brain 2020, 143, 2173–2188. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Caspers, S.; Moebus, S.; Lux, S.; Pundt, N.; Schutz, H.; Muhleisen, T.W.; Gras, V.; Eickhoff, S.B.; Romanzetti, S.; Stocker, T.; et al. Studying variability in human brain aging in a population-based German cohort-rationale and design of 1000BRAINS. Front. Aging Neurosci. 2014, 6, 149. [Google Scholar] [CrossRef]
- Herzog, H.; Langen, K.J.; Weirich, C.; Rota Kops, E.; Kaffanke, J.; Tellmann, L.; Scheins, J.; Neuner, I.; Stoffels, G.; Fischer, K.; et al. High resolution BrainPET combined with simultaneous MRI. Nuklearmedizin 2011, 50, 74–82. [Google Scholar] [PubMed]
- Langen, K.J.; Stoffels, G.; Filss, C.; Heinzel, A.; Stegmayr, C.; Lohmann, P.; Willuweit, A.; Neumaier, B.; Mottaghy, F.M.; Galldiks, N. Imaging of amino acid transport in brain tumours: Positron emission tomography with O-(2-[(18)F]fluoroethyl)-L-tyrosine (FET). Methods 2017, 130, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, M.; Beckmann, C.F.; Behrens, T.E.; Woolrich, M.W.; Smith, S.M. Fsl. Neuroimage 2012, 62, 782–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isensee, F.; Schell, M.; Pflueger, I.; Brugnara, G.; Bonekamp, D.; Neuberger, U.; Wick, A.; Schlemmer, H.P.; Heiland, S.; Wick, W.; et al. Automated brain extraction of multisequence MRI using artificial neural networks. Hum. Brain Mapp. 2019, 40, 4952–4964. [Google Scholar] [CrossRef] [Green Version]
- Pauleit, D.; Floeth, F.; Tellmann, L.; Hamacher, K.; Hautzel, H.; Muller, H.W.; Coenen, H.H.; Langen, K.J. Comparison of O-(2-18F-fluoroethyl)-L-tyrosine PET and 3-123I-iodo-alpha-methyl-L-tyrosine SPECT in brain tumors. J. Nucl. Med. 2004, 45, 374–381. [Google Scholar]
- Ashburner, J.; Friston, K.J. Unified segmentation. Neuroimage 2005, 26, 839–851. [Google Scholar] [CrossRef]
- Crinion, J.; Ashburner, J.; Leff, A.; Brett, M.; Price, C.; Friston, K. Spatial normalization of lesioned brains: Performance evaluation and impact on fMRI analyses. Neuroimage 2007, 37, 866–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, S.; Park, S.H.; Won, E.; Park, Y.R.; Kim, H.J. Propensity score matching: A conceptual review for radiology researchers. Korean J. Radiol. 2015, 16, 286–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berggren, R.; Nilsson, J.; Lovden, M. Education Does Not Affect Cognitive Decline in Aging: A Bayesian Assessment of the Association Between Education and Change in Cognitive Performance. Front. Psychol. 2018, 9, 1138. [Google Scholar] [CrossRef] [Green Version]
- Morris, J.C.; Heyman, A.; Mohs, R.C.; Hughes, J.P.; van Belle, G.; Fillenbaum, G.; Mellits, E.D.; Clark, C. The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology 1989, 39, 1159–1165. [Google Scholar] [PubMed]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- MacPherson, S.E.; Cox, S.R.; Dickie, D.A.; Karama, S.; Starr, J.M.; Evans, A.C.; Bastin, M.E.; Wardlaw, J.M.; Deary, I.J. Processing speed and the relationship between Trail Making Test-B performance, cortical thinning and white matter microstructure in older adults. Cortex 2017, 95, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Stuss, D.T.; Bisschop, S.M.; Alexander, M.P.; Levine, B.; Katz, D.; Izukawa, D. The Trail Making Test: A study in focal lesion patients. Psychol. Assess. 2001, 13, 230–239. [Google Scholar] [CrossRef]
- Kalbe, E.; Kessler, J.; Calabrese, P.; Smith, R.; Passmore, A.P.; Brand, M.; Bullock, R. DemTect: A new, sensitive cognitive screening test to support the diagnosis of mild cognitive impairment and early dementia. Int. J. Geriatr. Psychiatry 2004, 19, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.A. When to use the Bonferroni correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef]
- Salthouse, T.A. What cognitive abilities are involved in trail-making performance? Intelligence 2011, 39, 222–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuschmelting, V.; Weiss Lucas, C.; Stoffels, G.; Oros-Peusquens, A.M.; Lockau, H.; Shah, N.J.; Langen, K.J.; Goldbrunner, R.; Grefkes, C. Multimodal Imaging in Malignant Brain Tumors: Enhancing the Preoperative Risk Evaluation for Motor Deficits with a Combined Hybrid MRI-PET and Navigated Transcranial Magnetic Stimulation Approach. AJNR Am. J. Neuroradiol. 2016, 37, 266–273. [Google Scholar] [CrossRef] [Green Version]
- Weiss, C.; Tursunova, I.; Neuschmelting, V.; Lockau, H.; Nettekoven, C.; Oros-Peusquens, A.M.; Stoffels, G.; Rehme, A.K.; Faymonville, A.M.; Shah, N.J.; et al. Improved nTMS- and DTI-derived CST tractography through anatomical ROI seeding on anterior pontine level compared to internal capsule. Neuroimage Clin. 2015, 7, 424–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss Lucas, C.; Nettekoven, C.; Neuschmelting, V.; Oros-Peusquens, A.M.; Stoffels, G.; Viswanathan, S.; Rehme, A.K.; Faymonville, A.M.; Shah, N.J.; Langen, K.J.; et al. Invasive versus non-invasive mapping of the motor cortex. Hum. Brain Mapp. 2020, 41, 3970–3983. [Google Scholar] [CrossRef] [PubMed]
- Connor, M.; Karunamuni, R.; McDonald, C.; White, N.; Pettersson, N.; Moiseenko, V.; Seibert, T.; Marshall, D.; Cervino, L.; Bartsch, H.; et al. Dose-dependent white matter damage after brain radiotherapy. Radiother. Oncol. 2016, 121, 209–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujii, O.; Tsujino, K.; Soejima, T.; Yoden, E.; Ichimiya, Y.; Sugimura, K. White matter changes on magnetic resonance imaging following whole-brain radiotherapy for brain metastases. Radiat Med. 2006, 24, 345–350. [Google Scholar] [CrossRef]
- Szerlip, N.; Rutter, C.; Ram, N.; Yovino, S.; Kwok, Y.; Maggio, W.; Regine, W.F. Factors impacting volumetric white matter changes following whole brain radiation therapy. J. Neurooncol. 2011, 103, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Habets, E.J.J.; Hendriks, E.J.; Taphoorn, M.J.B.; Douw, L.; Zwinderman, A.H.; Vandertop, W.P.; Barkhof, F.; De Witt Hamer, P.C.; Klein, M. Association between tumor location and neurocognitive functioning using tumor localization maps. J. Neurooncol. 2019, 144, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Niki, C.; Kumada, T.; Maruyama, T.; Tamura, M.; Kawamata, T.; Muragaki, Y. Primary Cognitive Factors Impaired after Glioma Surgery and Associated Brain Regions. Behav. Neurol. 2020, 2020, 7941689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bullmore, E.; Sporns, O. The economy of brain network organization. Nat. Rev. Neurosci. 2012, 13, 336–349. [Google Scholar] [CrossRef]
- Park, H.J.; Friston, K. Structural and functional brain networks: From connections to cognition. Science 2013, 342, 1238411. [Google Scholar] [CrossRef] [Green Version]
- Wig, G.S. Segregated Systems of Human Brain Networks. Trends Cogn. Sci. 2017, 21, 981–996. [Google Scholar] [CrossRef] [Green Version]
- Galldiks, N. Contribution of PET imaging to radiotherapy planning and monitoring in glioma patients—A report of the PET/RANO group. Neuro-Oncology 2021. [Google Scholar] [CrossRef] [PubMed]
- Giuseppe, Z.R.; Silvia, C.; Eleonora, F.; Gabriella, M.; Marica, F.; Silvia, C.; Mario, B.; Francesco, D.; Savino, C.; Milly, B.; et al. Hippocampal-sparing radiotherapy and neurocognitive impairment: A systematic literature review. J. Cancer Res. Ther. 2020, 16, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Grosu, A.L.; Frings, L.; Bentsalo, I.; Oehlke, O.; Brenner, F.; Bilger, A.; Fennell, J.T.; Rothe, T.; Schneider-Fuchs, S.; Graf, E.; et al. Whole-brain irradiation with hippocampal sparing and dose escalation on metastases: Neurocognitive testing and biological imaging (HIPPORAD)—A phase II prospective randomized multicenter trial (NOA-14, ARO 2015-3, DKTK-ROG). BMC Cancer 2020, 20, 532. [Google Scholar] [CrossRef] [PubMed]
- Verma, V.; Robinson, C.G.; Rusthoven, C.G. Hippocampal-Sparing Radiotherapy for Patients with Glioblastoma and Grade II-III Gliomas. JAMA Oncol. 2020, 6, 981–983. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cognitive Function Domain/Test | Healthy Subjects (n = 121) | WHO Grade III/IV Glioma Patients (n = 121) | Patients Affected by Clinically Relevant Deficit a |
|---|---|---|---|
| Attention, processing speed [34,35] (TMT-A, seconds) | 30.9 (12.1) | 47.3 (33.9) *** | 39 (32%) |
| Processing speed/executive function (TMT-B, seconds) [34,35] | 68.2 (40.1) | 117.6 (80.2) *** | 34 (28%) |
| Executive function [36,37] (TMT-B/A ratio) | 2.25 (0.72) | 2.56 (0.94) ** | 19 (16%) |
| Language, word fluency [38] (supermarket, items) | 26.8 (4.4) | 20.2 (7.7) *** | 57 (47%) |
| Language processing [38] (number transcoding, items) | 3.6 (0.6) | 3.3 (1.1) n.s. | 21 (17%) |
| Verbal working memory [38] (digit span forward, weighted items) | 8.3 (2.3) | 7.4 (2.3) ** | 12 (10%) |
| Verbal working memory [38] (digit span backward, weighted items) | 8.0 (2.3) | 6.5 (2.5) *** | 20 (17%) |
| Visual working memory [38] (CBT forward, weighted items) | 7.4 (1.9) | 6.6 (2.3) * | 27 (22%) |
| Visual working memory [38] (CBT backward, weighted items) | 6.0 (2.0) | 4.8 (2.2) *** | 28 (23%) |
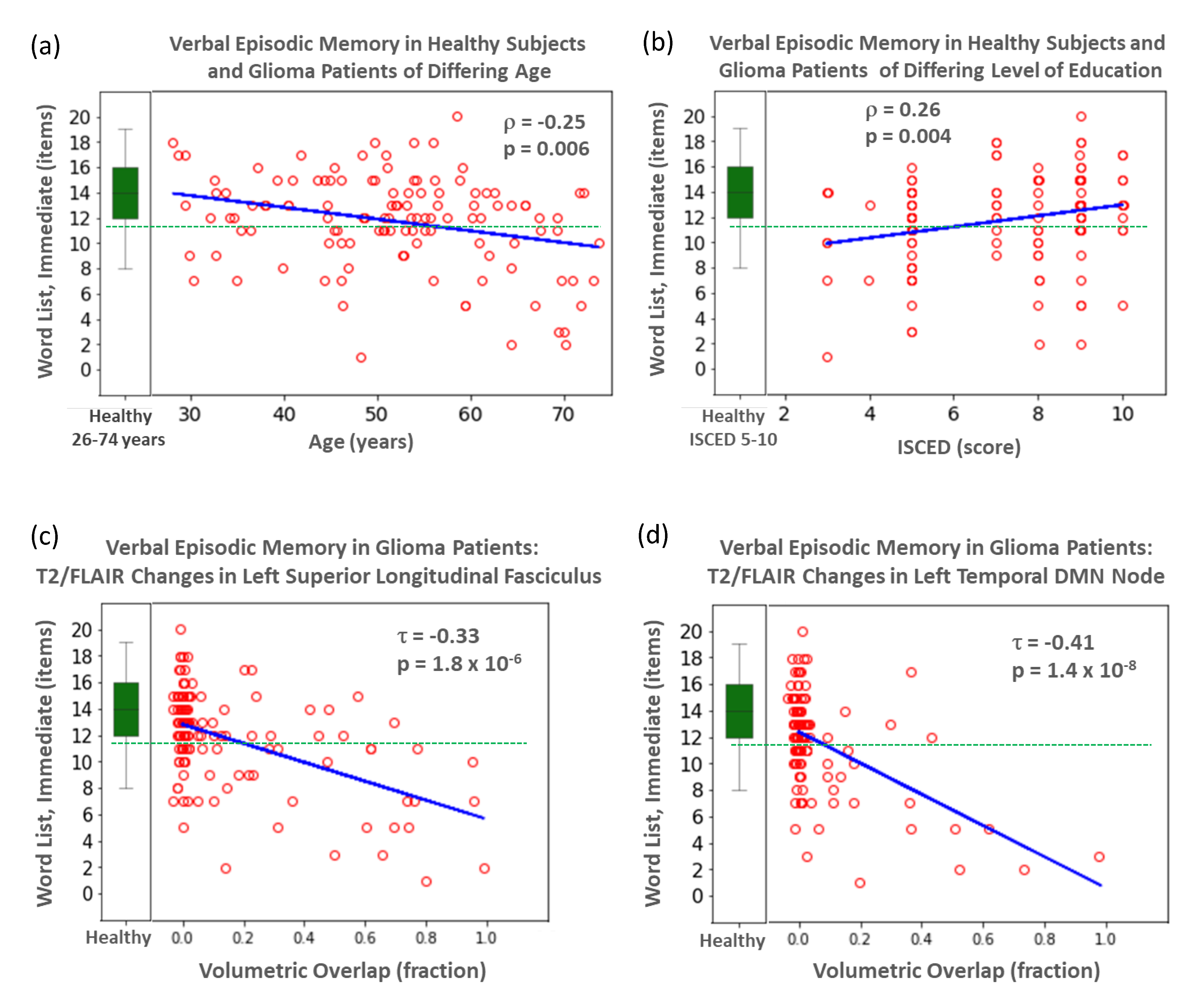
| Verbal episodic memory [38] (word list, immediate recall, items) | 14.1 (2.6) | 11.7 (3.7) *** | 34 (28%) |
| Verbal episodic memory [38] (word list, delayed recall, items) | 5.4 (2.4) | 4.5 (2.8) * | 22 (18%) |
| Cognitive Function Domain/Model Variables | Proportion Affected | Sens | Spec | PPV | NPV | ACC | AUC (ROC) | p (ROC) |
|---|---|---|---|---|---|---|---|---|
| Verbal Episodic Memory (Immediate Recall) | ||||||||
| Age + Edu + TotalVols | 0.28 | 0.21 | 0.95 | 0.64 | 0.75 | 0.74 | 0.56 | n.s. |
| + T2/FLAIR N25 | 0.28 | 0.35 | 0.95 | 0.75 | 0.79 | 0.79 | 0.67 | 0.013 # |
| Verbal Episodic Memory (Delayed Recall) | ||||||||
| Age + Edu + TotalVols | 0.18 | 0.18 | 0.98 | 0.67 | 0.84 | 0.83 | 0.58 | n.s. |
| + T2/FLAIR N33 | 0.18 | 0.45 | 0.98 | 0.83 | 0.89 | 0.88 | 0.72 | 0.01 # |
| Language (Number Transcoding) | ||||||||
| Age + Edu + TotalVols | 0.17 | 0.24 | 0.98 | 0.71 | 0.86 | 0.85 | 0.61 | n.s. |
| + T2/FLAIR T34 | 0.17 | 0.33 | 0.97 | 0.70 | 0.87 | 0.86 | 0.65 | 0.029 # |
| Executive Function (TMT A) | ||||||||
| Age + Edu + TotalVols | 0.32 | 0.49 | 0.90 | 0.70 | 0.79 | 0.77 | 0.70 | 0.001 |
| + T2/FLAIR T34 | 0.32 | 0.51 | 0.91 | 0.74 | 0.80 | 0.79 | 0.71 | 0.005 |
| Executive Function (TMT B) | ||||||||
| Age + Edu + TotalVols | 0.28 | 0.38 | 0.93 | 0.68 | 0.79 | 0.78 | 0.66 | 0.008 |
| + T2/FLAIR T34 | 0.28 | 0.35 | 0.99 | 0.92 | 0.80 | 0.81 | 0.67 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kocher, M.; Jockwitz, C.; Lohmann, P.; Stoffels, G.; Filss, C.; Mottaghy, F.M.; Ruge, M.I.; Weiss Lucas, C.; Goldbrunner, R.; Shah, N.J.; et al. Lesion-Function Analysis from Multimodal Imaging and Normative Brain Atlases for Prediction of Cognitive Deficits in Glioma Patients. Cancers 2021, 13, 2373. https://doi.org/10.3390/cancers13102373
Kocher M, Jockwitz C, Lohmann P, Stoffels G, Filss C, Mottaghy FM, Ruge MI, Weiss Lucas C, Goldbrunner R, Shah NJ, et al. Lesion-Function Analysis from Multimodal Imaging and Normative Brain Atlases for Prediction of Cognitive Deficits in Glioma Patients. Cancers. 2021; 13(10):2373. https://doi.org/10.3390/cancers13102373
Chicago/Turabian StyleKocher, Martin, Christiane Jockwitz, Philipp Lohmann, Gabriele Stoffels, Christian Filss, Felix M. Mottaghy, Maximilian I. Ruge, Carolin Weiss Lucas, Roland Goldbrunner, Nadim J. Shah, and et al. 2021. "Lesion-Function Analysis from Multimodal Imaging and Normative Brain Atlases for Prediction of Cognitive Deficits in Glioma Patients" Cancers 13, no. 10: 2373. https://doi.org/10.3390/cancers13102373