Origin, Fate and Control of Pharmaceuticals in the Urban Water Cycle: A Case Study
by

Roberta Hofman-Caris
1, 
Thomas ter Laak
1,
Hans Huiting
1,
Harry Tolkamp
1,2,
Ad de Man
3,
Peter van Diepenbeek
4 and
Jan Hofman
5,*
1
KWR Watercycle Research Institute, PO Box 1072, 3430 BB Nieuwegein, The Netherlands
2
Waterschap Limburg, PO box 2207, 6040 CC Roermond, The Netherlands
3
Waterschapsbedrijf Limburg, PO Box 1315, 6040 KH Roermond, The Netherlands
4
Waterleiding Maatschappij Limburg, PO Box 1060, 6201 BB Maastricht, The Netherlands
5
Department of Chemical Engineering, Water Innovation and Research Centre, University of Bath, Claverton Down, Bath BA2 7AY, UK
*
Author to whom correspondence should be addressed.
Water 2019, 11(5), 1034; https://doi.org/10.3390/w11051034
Submission received: 28 April 2019
/
Revised: 12 May 2019
/
Accepted: 15 May 2019
/
Published: 17 May 2019
(This article belongs to the Special Issue Removal of Pharmaceuticals from Water: Conventional and Alternative Treatments)
Abstract
:The aquatic environment and drinking water production are under increasing pressure from the presence of pharmaceuticals and their transformation products in surface waters. Demographic developments and climate change result in increasing environmental concentrations, deeming abatement measures necessary. Here, we report on an extensive case study around the river Meuse and its tributaries in the south of The Netherlands. For the first time, concentrations in the tributaries were measured and their apportionment to a drinking water intake downstream were calculated and measured. Large variations, depending on the river discharge were observed. At low discharge, total concentrations up to 40 μg/L were detected, with individual pharmaceuticals exceeding thresholds of toxicological concern and ecological water-quality standards. Several abatement options, like reorganization of wastewater treatment plants (WWTPs), and additional treatment of wastewater or drinking water were evaluated. Abatement at all WWTPs would result in a good chemical and ecological status in the rivers as required by the European Union (EU) Water Framework Directive. Considering long implementation periods and high investment costs, we recommend prioritizing additional treatment at the WWTPs with a high contribution to the environment. If drinking water quality is at risk, temporary treatment solutions in drinking water production can be considered. Pilot plant research proved that ultraviolet (UV) oxidation is a suitable solution for drinking water and wastewater treatment, the latter preferably in combination with effluent organic matter removal. In this way >95% of removal of pharmaceuticals and their transformation products can be achieved, both in drinking water and in wastewater. Application of UV/H2O2, preceded by humic acid removal by ion exchange, will cost about €0.23/m3 treated water.
1. Introduction
Organic micropollutants in water have been a topic of interest for some time [1]. They include industrial compounds, pesticides, personal care products, steroid hormones and pharmaceuticals (both from human and veterinary consumption). The presence of pharmaceutical compounds in surface waters was suspected and proven already long ago [2,3]. More recently, it became apparent that many different pharmaceutical compounds are found in surface water and groundwater [4]. It is expected that the environmental numbers and concentrations will increase, because new pharmaceuticals are being developed and pharmaceutical consumption is increasing due to demographic changes such as growing and aging populations [5]. Another factor that probably will affect the pharmaceutical concentration in surface waters, is climate change, which in The Netherlands and Western Europe is expected to cause longer dry periods—the summer of 2018 was a good example—and thus higher concentrations of micropollutants in surface waters (less dilution) will occur [6,7].
Most of the pharmaceuticals and their metabolites are excreted from the body via urine and feces after use. They are transported to wastewater treatment plants (WWTPs), where they are discharged into the environment. To protect receiving surface waters, these WWTPs apply biological processes to remove organics, nitrogen and phosphorous from the wastewater, but they are not specifically designed to remove organic micropollutants, including pharmaceuticals. In practice, the removal of the organic micropollutants varies between 0% and 100%, with an average total removal of 60%–70%. As a result, significant pharmaceuticals concentrations are present in WWTP effluent and will end up in surface waters and, therefore, in sources for drinking water production [8].
As these biologically active compounds are designed to bring about a specific effect in organisms, there is an increasing understanding that the presence of pharmaceuticals in surface water is undesired [9,10,11]. It already has been shown that some of these compounds, like diclofenac, fluoxetine and hormone disruptors can change the behavior of predators in water and can accumulate through the food chain [12]. Others reported on fish feminization and reduced reproduction [9].
For drinking water, the risk for human health of individual compounds at low concentrations is negligible. However, little is known about the effects of long-term exposure to pharmaceutical mixtures. Furthermore, Dutch drinking water utilities have the policy of distributing impeccable water quality, which means that from a precautionary principle, pharmaceuticals and other micropollutants should in principle be absent in drinking water.
Because of the environmental concerns, the EU has developed a watch list that includes 17-beta-estradiol (E2), 17-alpha-ethinylestradiol (EE2), and diclofenac. It is expected that eventually standards will be set for these compounds [13,14]. The currently proposed revision of the European Union (EU) Drinking Water Directive [15], contains several new standards for chemical parameters, including beta-estradiol, and some endocrine disrupters.
Drinking water utilities and authorities for managing surface water quality are, therefore, looking for adequate solutions for protecting of surface water quality, sources for drinking water and the production of high-quality drinking water, free of pharmaceuticals and micropollutants. There are three approaches that can contribute to this: (1) prevent emissions by reducing consumption and removal at source, (2) removal during wastewater treatment, and (3) removal during drinking water treatment.
The first option would be the most elegant solution to prevent pharmaceuticals from entering the wastewater and the environment. However, people cannot be denied the use of medication. It would already have a large impact if the public and especially physicians would realize that pharmaceuticals are not harmless, and that in some cases it may be better to prescribe an alternative pharmaceutical or lower dose, to protect the environment [16,17]. This, however, will not result in the absence of pharmaceuticals and their metabolites in wastewater, and additional treatment in WWTP and/or drinking water treatment may become inevitable in future. Currently activated carbon adsorption or oxidation by ozone are considered as the current industry standard for this purpose, but these technologies come with high costs. Nanofiltration or reversed osmosis is not favored, as it is difficult to discharge the concentrates. Advanced oxidation processes (AOPs) do not have this disadvantage. The application of AOPs in wastewater treatment has been studied by several authors. In The Netherlands, where bromide concentrations on the average are about 120 μg/L in the Rhine and about 70 μg/L in the Meuse, where they enter the country [18], this would result in a significant increase in the bromate content of surface water. This is an unwanted side effect, as bromate is considered carcinogenic. Varanasi, Coscarelli et al. (2018) [19] studied ultraviolet (UV)/H2O2, UV/free chlorine and UV/persulfate processes (UV/PS) for the removal of trace organic compounds, and concluded that their efficiency is greatly affected by the presence of background dissolved organic matter (DOM). The performance of UV/H2O2 and UV/free chlorine processes is mainly affected by DOM containing more aliphatic components, whereas the performance of UV/PS mainly depends on the presence of aromatic compounds.
According to Nihemaiti et al. (2018) [20] UV/peroxydislufate (UV/PDS) processes are more effective than UV/H2O2 processes for the removal of trace organic compounds in pure water. However, electron-rich compounds in effluent organic matter (EfOM) will cause high competition in UV/PDS processes. Thus, the efficiency of UV/PDS strongly depended on the variation of the composition and concentration of DOM and nitrite. In general, higher UV fluences and oxidant doses were required to overcome the impact of the water matrix. Application of UV/H2O2 does not result in the formation of byproducts from H2O2, but in case of UV/PDS processes, the effect of the resulting sulfate concentration on salinity should be considered. Application of different AOPs for the treatment of municipal wastewater has also been evaluated by other authors [21,22,23]. In general UV/free chlorine processes show a better performance than UV/H2O2 processes, although UV/chlorine processes show a higher compound selectivity. The same conclusion was drawn by Guo et al. [24], who found that UV/chlorine processes are less affected by the water and wastewater matrices than UV/H2O2 processes (which are superior in pure water, if compounds are more sensitive towards hydroxyl radicals). However, in The Netherlands chlorine-based processes are not preferred because of the possible formation of chlorine containing byproducts. According to Miklos et al. [21], the efficiency of UV/H2O2 processes in wastewater treatment strongly depends on the nitrite concentration, and the matrix composition should be monitored for effective application of UV/H2O2 processes.
This paper presents a case study in the province of Limburg in The Netherlands, comprising the river Meuse and several tributaries, upstream from the drinking water production plant ‘Heel’, which uses the river water as a source. The study area comprises several wastewater treatment plants, with direct influence on the water quality of the intake of the drinking water plant. The origin and fate of pharmaceuticals and metabolites in the study area are assessed, as well as different abatement options for water-quality control. Data for this study were acquired from a broader national wastewater effluent survey and two pilot plant investigations. The novelty of the study is in its integrated character and bridging between drinking water production and source control. In The Netherlands, drinking water production and surface water management are traditionally separated and independent sectors.
The goal of this integrated study was to develop and compare practical and cost-effective solutions for tackling pharmaceuticals in the drinking water produced at Heel and the surface water quality in the study area and at the raw water intake. The criteria for evaluation are water quality, environmental benefits, required time for realization and costs.
2. Materials and Methods
2.1. General Approach and Data Used in This Study
The central point of the study was the drinking water production from surface water from the river Meuse at the treatment plant in Heel. The focus of this study is on the presence of pharmaceuticals and metabolites in the river water, and the direct influence of WWTP emissions in the upstream catchment area on the intake for the drinking water production. As abatement options, the application of advanced oxidation processes for drinking water or wastewater treatment were evaluated.
The evaluations and assessments done in this paper are based on the results of three underlying studies in collaboration with the drinking water company “Waterleiding Maatschappij Limburg”, the water board “Waterschap Limburg”, responsible for the surface water quality in the area, and the wastewater treatment operator “Waterschapsbedrijf Limburg”. In addition, data from a national survey of effluent quality were used. Sampling and data collection took place in different time periods. Therefore, some differences in investigated contaminants occur in the different phases of this integrated study.
The approach followed in this study comprises of the following steps:
- Assessment of concentrations of pharmaceuticals and metabolites in several wastewater treatment effluents throughout The Netherlands to provide contextual or reference data for comparison with the effluents in the study area.
- Assessment of loads and concentrations of pharmaceuticals in the river Meuse and tributaries upstream of the drinking water intake of treatment plant Heel. This includes the apportionment of the contribution of pharmaceuticals of the different wastewater treatment plants in the study area to the drinking water intake.
- Evaluating different abatement options for pharmaceuticals and metabolites in the study area, including options for drinking water treatment and wastewater treatment. The focus is on the application of advanced oxidation processes.
- Finally, a vision for short term and longer-term solutions is presented.
The sections below describe the study area, the national sampling campaign, and the pilot plant studies for drinking water treatment and wastewater treatment with AOP.
2.2. Study Area and Sampling Points
The area studied in this paper is the river basin of the river Meuse, upstream from the water intake of the drinking water production plant Heel. The Meuse rises at the French Plateau de Langres and flows through Belgium, after which it enters The Netherlands at the town of Eijsden. The river basin upstream of the intake of water production plant Heel (WPH) counts about six million inhabitants, of which 5.3 million are in Belgium and France. For this research and drinking water production, the following tributaries are of importance: The Jeker (95% flowing through Belgium), the Geul (50% flowing through Belgium), the Geleenbeek (100% Netherlands), and the Slijbeek (partly Belgium).
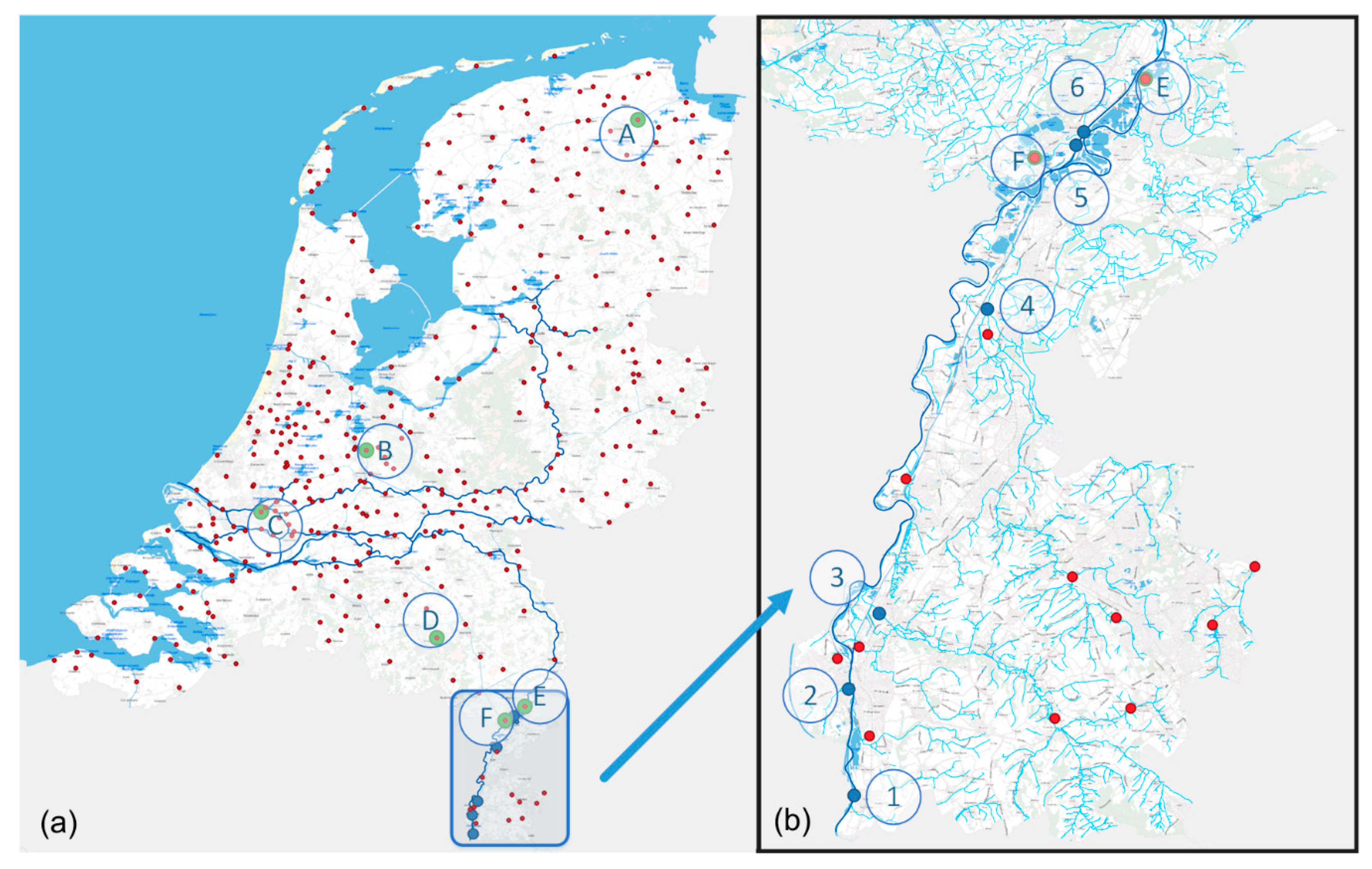
An inventory was made of pharmaceuticals in surface water and in the effluent of several wastewater treatment plants (WWTPs) [25]. In winter 2011 samples were taken in 4 consecutive weeks at 6 different locations in the river Meuse and its tributaries in the southern part of Limburg and in a canal parallel to the Meuse (the “Lateraal Kanaal”). Sample locations (See Figure 1b) were ① Eijsden (near the Belgian-Dutch border), ② the river Jeker in Maastricht, near the place where it enters the Meuse, ③ the river Geul near Meerssen, ④ the Geleenbeek near Oud Roosteren, ⑤ the Slijbeek, near the place where it enters the Lateraal Kanaal, and ⑥ at the intake of the drinking water production site Heel, which uses surface water from the Lateraal Kanaal as a source. The samples were single grab samples taken from bridges. The first two samples were taken at the end of a very long dry period (6 months) with a very low discharge flow in the Meuse. After the second sampling, rainfall commenced, the discharge flow increased. The third and fourth samples were, therefore, taken during a higher river discharge. See Supplementary Information for details Figures S1–S7 for details of the sampling points and the hydrograph.
2.3. National Sampling Campaign
In the national sampling campaign, effluent samples were taken at the WWTPs of Garmerwolde (A), Utrecht (B), Rotterdam (C), Eindhoven (D), Panheel (E) and Roermond (F) (see Figure 1a). Samples were single samples collected with an automatic sample collector over 24 h and proportional to the effluent flow rate, under dry weather conditions. In the WWTP effluent total organic carbon (TOC), dissolved organic carbon (DOC), and UV-Transmittance (UV-T254) at 254 nm were measured at the KWR laboratory. Composition of effluent organic matter (EfOM) was analyzed by DOC-Labor Dr. Huber (Eisenbahnstr. 6, 76229 Karlsruhe, Germany), applying an LC-OCD method [26]. The pharmaceuticals studied were selected based on consumption, occurrence in the environment, physico-chemical properties, the availability of standards and analytical methods [27]. Concentrations of pharmaceuticals and metabolites in surface water and WWTP effluents were measured according to the ultra-high performance liquid chromatography–tandem mass spectrometry (UPLC-MS/MS) method described previously Wols et al. [28].
2.4. Wastewater Treatment Pilot Plant Panheel
To study the effect of additional treatment, experiments were carried out in a pilot set-up at WWTP Panheel, in which a mixture of more than 40 pharmaceuticals was dosed to the effluent to be able to study the removal efficiency of the additional treatment. The compounds were selected based on their presence in WWTP effluents and surface waters. The pilot plant comprised of a multi-layer filter (proprietary filter material; PureBlue Water, Kapellebrug, The Netherlands) to remove suspended solids and particles, an anion exchange (IEX) unit containing Lewatit S6368A resin (Lanxess, Brussels, Belgium) to remove humic acids, and a UV reactor (Type M3 by PureBlue Water; Kapellebrug, The Netherlands), which, after addition of H2O2 to the solution, was operated at a dose of 150 or 300 mJ/cm2 for a UV/H2O2 process. The UV reactor was equipped with a low-pressure Amalgam lamp of 90 W. A largely over-dimensioned granular activated carbon (GAC) filtration unit filled with Norit GAC (type PK 1-3; Cabott Norit Netherlands, Amersfoort, The Netherlands) was used to prevent any discharge of added pharmaceuticals to the surface water. Further details on the pilot set-up can be found in Hofman-Caris et al. [29].
2.5. Drinking Water Treatment Pilot Plant Heel
The experiments at drinking water treatment plant Heel were carried out in a pilot set-up as described by Hofman-Caris et al. [27]. The flow through the reactor was 1–2.5 m3/h. The UV reactor (type D200, Van Remmen UV-Techniek, Wijhe, The Netherlands) was optimized for advanced oxidation reactions according to [30]. It had been equipped with one LP UV lamp (Heraeus NNI 125-84-XL, Hanau, Germany) and two baffles to improve the flow conditions. Here too the mixture of over 40 pharmaceuticals and a H2O2 solution were added to the influent of the UV reactor. Again, a largely over-dimensioned granular activated carbon (GAC) filtration unit was used to prevent any discharge of added pharmaceuticals to the environment.
3. Results
3.1. Analysis of Wastewater Treatment Plant (WWTP) Effluents
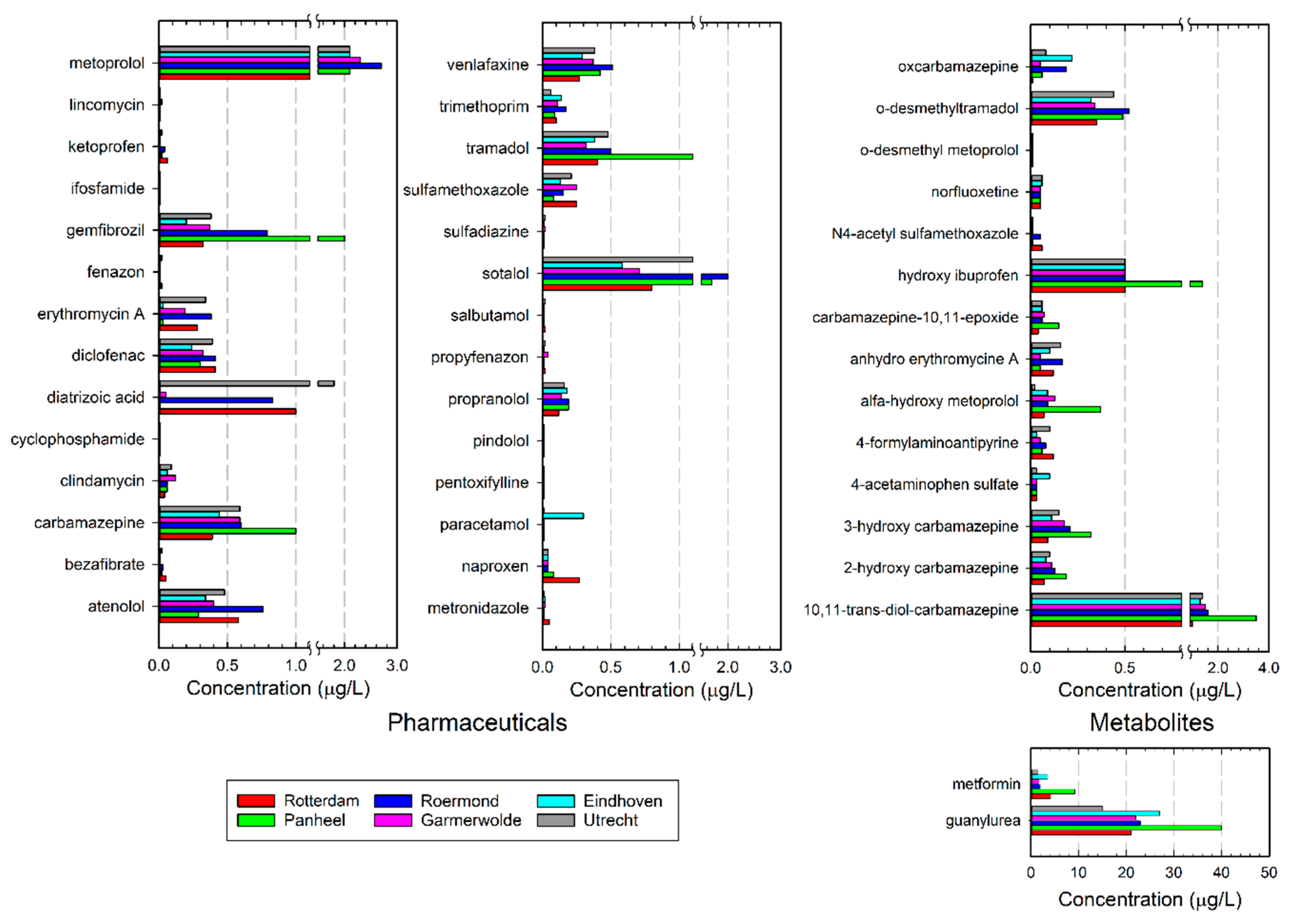
The presence of pharmaceuticals in various WWTP effluents throughout The Netherlands is shown in Figure 2.
From these data it can be concluded that there are large differences in the presence of certain pharmaceuticals in the effluent of various WWTPs. These differences can have several causes: e.g., sampling conditions, and diurnal and seasonal patterns can affect the observed concentrations. Removal efficiencies may vary too. Some compounds, like sotalol, were found in relatively high concentrations in the effluent of Utrecht, Roermond and Panheel (1.5–2.0 μg/L), whereas concentrations were smaller in Eindhoven, Garmerwolde and Rotterdam (0.5–0.8 μg/L). In contrast, diclofenac (0.24–0.41 μg/L) and venlafaxine (0.27–0.51 μg/L) had similar concentrations in all WWTP effluents analyzed. Tramadol, gemfibrozil, and carbamazepine were found in relatively high concentrations in the Panheel effluent, whereas in Utrecht a high concentration of diatrizoic acid was observed. In general, the effluents contained 14–28 μg/L of total pharmaceuticals and metabolites included in the analytical procedure, the average total pharmaceuticals concentration being about 16 μg/L. In the Panheel effluent the average concentration, however, was about 28 μg/L, which is relatively high. This is probably caused by the relatively high contribution of a nursing home, which sends its wastewater to this rather small WWTP. Such factors may also affect the presence of individual pharmaceuticals in the effluent, which confirms earlier findings of the ZORG project in The Netherlands [31].
The data also indicate that some pharmaceuticals can easily be removed by the WWTP (like paracetamol, sulfadiazine, cyclophosphamide, norfluoxetine, lincomycin, phenazone, cyclophosphamide, bezafibrate, sulphadiazine, salbutamol, propyphenazone, pentoxyfylline and metronidazole), whereas others are very difficult to remove (like diatrizoic acid, metoprolol and diclofenac). Carbamazepine is partly converted, either by the human metabolism or by biodegradation. Several transformation products of carbamazepine (oxcarbamazepine, carbamazepine-10,11-epoxide, 2-hydroxy carbamazepine, 3-hydroxy carbamazepine, and 10,11-trans-diol carbamazepine) could be detected. Also, for tramadol and ibuprofen, transformation products can be found. Metformin is an antidiabetic that is present in high concentrations in wastewater because it is prescribed in high daily dosages to a large part of the population. In the WWTP metformin is converted by means of biodegradation into guanylurea, which is very difficult to further degrade in a WWTP. As a result, the concentrations of metformin and guanylurea are very high: in general, their concentrations are above 10 μg/L; in Panheel concentrations up to 40 μg/L were observed. Although often considered relatively harmless, metformin can act as an endocrine disruptor at environmentally relevant concentrations [32,33].
3.2. Pharmaceutical Loads in Surface Waters
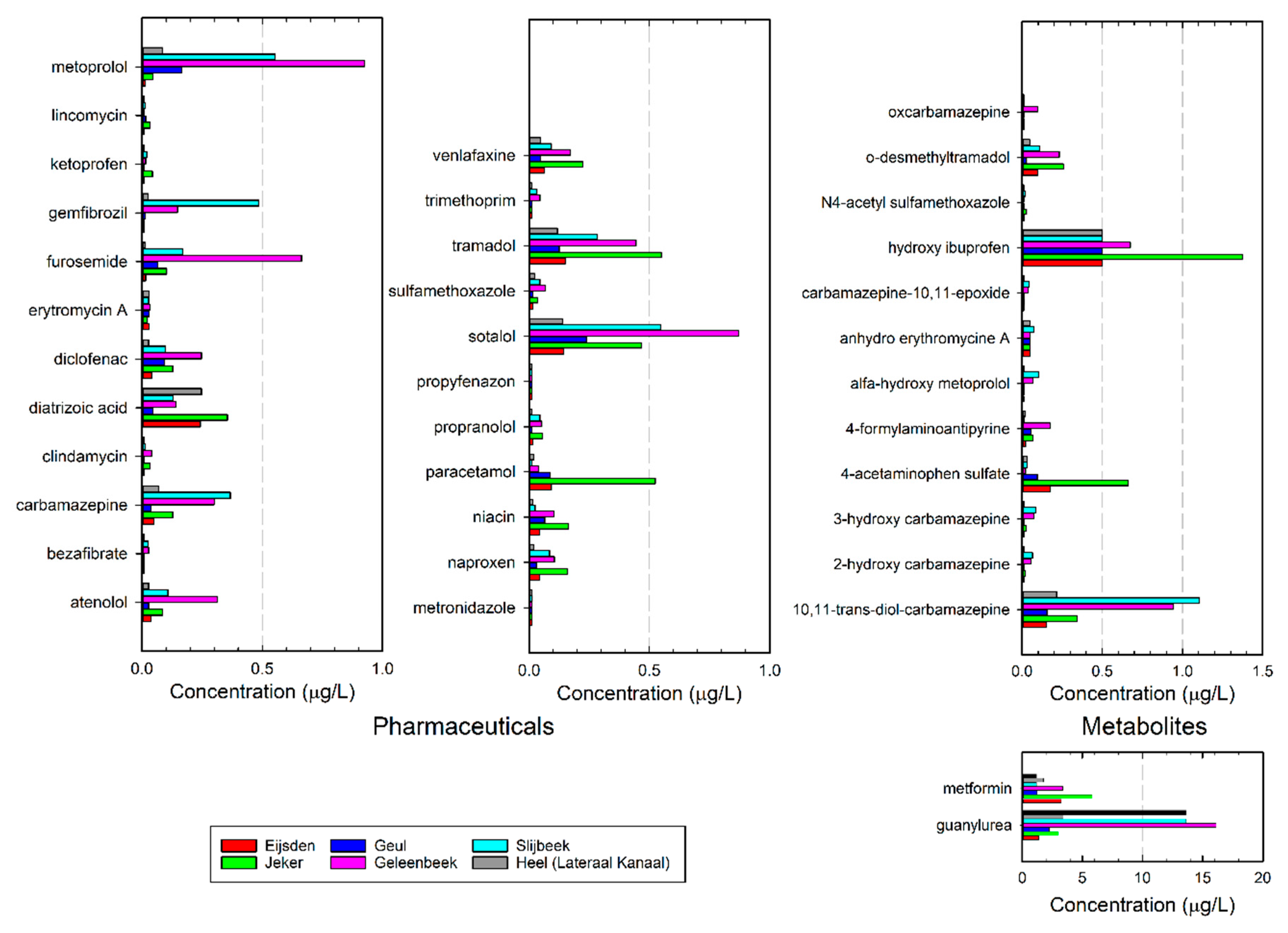
The concentrations found in the WWTPs are a strong indication that WWTP effluent significantly contributes to the pharmaceutical load in surface waters. This is confirmed by the pharmaceuticals’ concentrations found in the Meuse and its tributaries, as shown in Figure 3. Here the average concentration of four measurements (two in November, and two in December) is shown. The full data set can be found in the Supplementary Information (Tables S1–S12).
The pharmaceuticals load in the Meuse crossing the border between Belgium and The Netherlands strongly depends on the river discharge, which can vary almost two orders of magnitude. The minimum discharge at Eijsden is about 10 m3/s, the nominal flow 147 m3/s, whereas the maximum discharge is about 1400 m3/s (period 2005–2009). In the most extreme situations, the discharge can even be as high as 3000 m3/s. As the discharge of the Meuse depends on the rainfall in its catchment area, dry periods with low discharge up to six months may occur. The pharmaceutical load of the Meuse in Eijsden was calculated from the measured concentrations and the river discharge of 14 m3/s (November 2011) and of 253 m3/s (December 2011) (See discharge graph in the supplementary information, Figure S7). This resulted in an average load of 10 kg/day (standard deviation 18%) under low discharge conditions, and of 106 kg/day (standard deviation 32%) under higher discharge conditions. The load in the high-flow condition is higher than one would expect based on dilution. This is most probably caused by a ‘first-flush’ effect. The concentrations were measured at the initial flank of a rapidly increasing discharge: the flow was already high, but water with high concentrations was pushed forward in the river, without dilution.
Figure 3 shows the pharmaceuticals concentrations present in the various tributaries. In the Jeker, Geleenbeek and Slijbeek concentrations were higher than in the Meuse, due to the high load of WWTP effluent in these tributaries. WWTP effluent forms a significant part of the total discharge in these tributaries, as shown in Table 1. The WWTP of Panheel (25,000 PE) discharges to the Slijbeek and the WWTPs of Susteren (216,500 PE), Hoensbroek (240,000 PE) and Heerlen (65,600 PE) discharge to the Geleenbeek, resulting in relatively high pharmaceutical concentrations. In the Geleenbeek and the Slijbeek, the river discharge originated for roughly 40–50% from effluent. The amount of wastewater in the Jeker could not be quantified because of an unknown but significant contribution of untreated municipal wastewater from Belgium [34]. It is estimated that the wastewater of about 120,000 Belgian inhabitants is discharged at the Jeker. About one third of this had not or limitedly been treated (Situation 2011). Instead, a bacterial suspension is added to the river to improve water quality. Pharmaceutical concentrations in the Jeker appear to be a little lower than in the Geleenbeek and the Slijbeek.
Metformin is converted to guanylurea by biodegradation during biological wastewater treatment. The fact that in the Jeker at the time of the measurement a relatively large contribution of untreated wastewater was found probably accounts for the high contribution of metformin compared with its metabolite guanylurea. Furthermore, the concentrations of some painkillers and their transformation products (tramadol, paracetamol, acetaminophen sulphate, and ibuprofen) are higher in the Jeker than in other surface waters. This may be related to differences in the pharmaceutical use between The Netherlands and Belgium but can also result from a larger contribution of untreated wastewater, in which these compounds were not removed. The concentration in the Geul is the lowest, because of the relatively low contribution of effluent on the river discharge.
Ter Laak et al. [35] combined data on the flow of different rivers and demographics of the catchments to calculate daily per capita loads of pharmaceuticals and metabolites. Subsequently, they linked these loads to sales data of pharmaceuticals in the catchment and, considering human excretion and removal by WWTPs, thus were able to predict actual loads within a factor of three for most pharmaceuticals. Furthermore, from this study it became clear that there are differences in the use of pharmaceuticals per capita in The Netherlands and Belgium: the Jeker contains relatively high concentrations of metformin, diatrizoic acid, venlafaxine, tramadol, paracetamol, niacin, and naproxen. Also, the study by Ter Laak et al. [35] revealed differences in prescription practice between the two countries. Furthermore, the river is strongly affected by WWTP effluent and—at the time of the research—untreated municipal wastewater from Belgium.
3.3. Abatement Options to Protect Surface Water Quality and Drinking Water Production
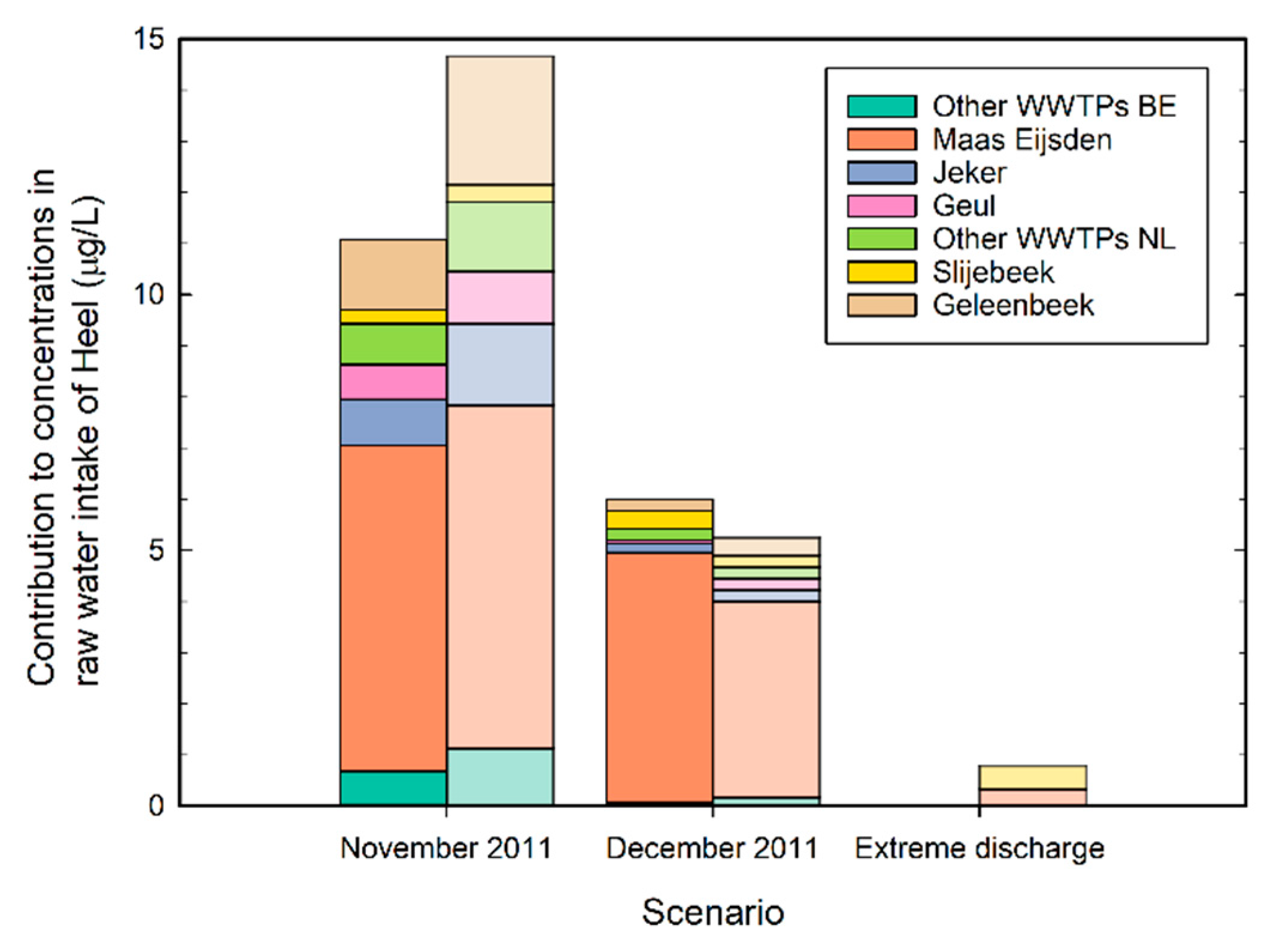
The estimated contribution of the Meuse and its tributaries to the concentration of pharmaceuticals and metabolites in the intake of drinking water production site Heel is shown in Figure 4. The darker shaded bars for November and December are based on loads predicted from the actual measurement in these months. The lighter bars are based on load predictions for extreme low, median and extreme high discharge. As expected, the river Meuse has the largest contribution to the intake, especially in median- and high-discharge situations. At extreme high flow it is also observed that the concentrations will be low due to dilution. However, during low flow, which can take up to 6 months in dry years, the direct contributions of the tributaries to the drinking water intake are large, up to almost 50%. Treatment measures on the WWTPs along the tributaries can effectively reduce the pharmaceutical compounds in the intake for drinking water production.
As it is expected that the pharmaceutical loads and concentrations will increase in the future, several abatement options were studied to control surface water quality and/or prevent concentrations that are too high in drinking water.
Table 2 gives an overview of the possibilities, their expected effects and the estimated operational costs. The options will be described in more detail below. The first abatement option in Table 2 is reducing the emission of pharmaceuticals at the source. This is not easy to realize. People need pharmaceuticals because of health problems, and it is not ethical to abstain pharmaceuticals only because of environmental reasons. In many cases, alternative pharmaceuticals will probably show comparable behavior in the environment, as the activity of a compound is strongly related to its chemical structure, which, as a result, will show strong resemblances. In some cases, physicians can prescribe different pharmaceuticals (like naproxen instead of diclofenac) or minimize doses.
The second option is to divert effluent by realizing a different layout of the water system, combining some WWTPs, or relocating them downstream of the drinking water intake. This may be effective for the quality improvement of the local intake water of the drinking water production, but for the total aquatic environment, it is not effective, as the same load of pharmaceuticals and metabolites eventually will end up in the surface water. Moreover, there will be no change for drinking water intakes further downstream. For the situation in Heel this could be an option that is easy to realize, because WWTP Panheel discharges via the Slijbeek into the Lateraal Kanaal, a few hundred meters upstream of the raw water intake of WPH.
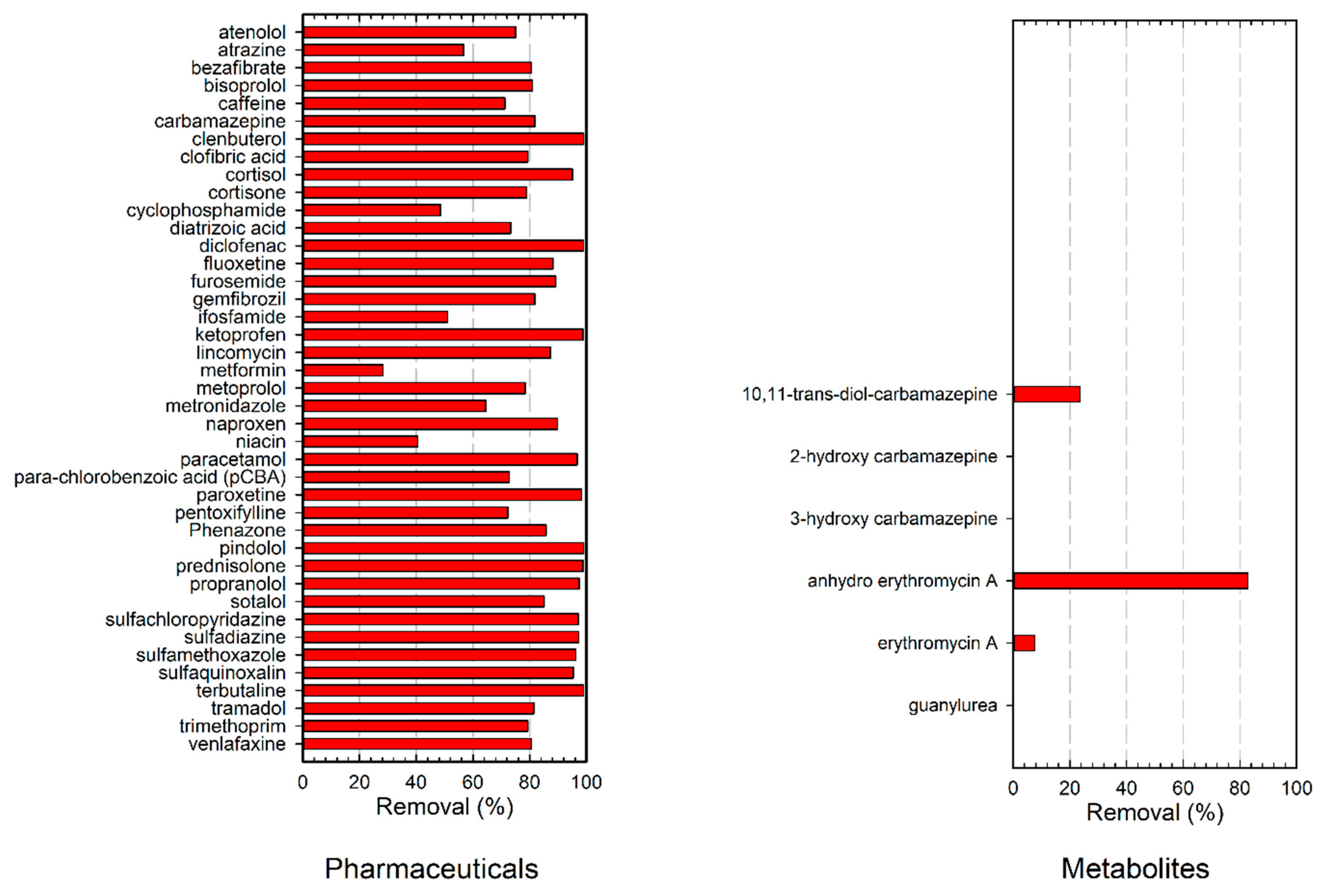
The third option, extension of individual WWTPs with additional treatment steps, will be very effective for the local aquatic environment [36]. Some pilot experiments were carried out at WWTP Panheel [29]. It was shown that the effectiveness of advanced oxidation, e.g., based on UV/H2O2 processes, can very much be improved by first removing the humic acid part of the effluent organic matter by means of ion exchange. In general, UV/H2O2 processes have a high energy demand, but removal of the humic acids increased the UV-transmission from 38% to 85% resulting in an 84% reduced energy demand. Furthermore, most pharmaceuticals were broken down >85% (Figure 5). Interestingly, a UV dose of 150 mJ/cm2, combined with a H2O2 concentration of 10 mg/L, seems to be quite effective. This is a much lower dose than commonly applied for advanced oxidation of contaminants in drinking water (often about 500 mJ/cm2). Hence, the costs of UV/H2O2, preceded by humic acid removal by ion exchange, will be relatively low at about €0.23/m3 treated water.
The main disadvantage of this system is the fact that it only results in a very local improvement of the aquatic environment, and thus only will be effective if it is applied at a large scale, involving many or all WWTPs. Furthermore, in the actual situation in the study area, the largest load of pharmaceuticals is present in the Meuse already before it enters The Netherlands. Therefore, only adjusting the Dutch WWTPs will not be very effective at improving the total surface water quality. Nevertheless, the contribution of the tributaries can be significant in dry periods as can be seen in Figure 4. These dry periods are more likely to occur in future and last longer, due to climate change, and these dry periods result in the highest concentrations and associated risk [7]. To obtain an effective reduction of the load all, or at least the majority, of WWTPs in the catchment area require additional treatment. Depending on what needs protection, smart abatement solutions can be developed [37]. This is indicated by the fourth option in Table 2. In that case the total surface water quality, and thus also the source water quality for drinking water production would be significantly improved. However, this will involve considerable investments and solutions have to be found in international cooperation, since the rivers cross borders.
The final solution, option five, may be additional treatment at the point of drinking water production. This has been tested for the situation in Heel, applying advanced oxidation (UV/H2O2) [27]. As the UV-transmission of the intake water already is high (94%) due to the river bank filtration, this process is very effective, removing >90% of most pharmaceuticals (Figure 6). By optimizing the reactor geometry, it was shown that even in this case significant improvement of the process efficiency (a 40% decrease in energy demand) could be obtained. Due the very high UV transmittance of the influent of the UV reactor, reflection of UV irradiation at the outer reactor wall occurred. As a result, in the pilot set-up applied, the actual UV dose could not be decreased below 365 mJ/cm2, but obviously, for practical applications a lower UV dose would have been sufficient, as most pharmaceuticals were removed to a high degree. Metabolites in general were also removed, although for 3-hydroxy carbamazepine formation of about 25 μg/L could be observed, probably due to the conversion of carbamazepine by the Advanced Oxidation Processes).
A drawback of this fifth option is that, although it can significantly improve drinking water quality in the case of increasing pharmaceutical concentrations, it does not affect surface water quality and thus the aquatic environment.
4. Discussion
The above case study in Limburg has indicated that pharmaceuticals and metabolites can be present in surface water in relatively high concentrations in the study area. The concentrations are largely influenced by the river discharge flow and are expected to increase in future due to demographic changes and prolonged dry periods. In these dry periods in particular, concentrations are high in the tributaries and the raw water intake of the drinking water production. This is an undesired situation from a precautionary perspective for drinking water quality and aquatic life.
Different abatement options have been considered in this case study ranging from changes in the water system to the use of additional treatment technology for drinking water and wastewater treatment. It was concluded that the best measure would be to remove pharmaceuticals on all WWTPs in the catchment. This would reduce concentrations of pharmaceuticals in the river system significantly, creating a good chemical and ecological status, and it would make additional treatment in the drinking water production superfluous. In this way the system could comply perfectly with the regulations of the Water Framework Directive. However, the investment costs would be high and international collaboration is required, probably making this a long-term solution [36,38].
The methodology presented here to identify the origin and fate of pharmaceutical compounds can be used to identify WWTPs that act as hotspots for pollution. At these hot-spots, additional treatment technology could be installed with priority to improve the surface water quality in the receiving water bodies. If during the development of this abatement option the drinking water quality still would be at risk, temporary additional treatment at the drinking water production point could be considered. These temporary measures should always be considered in an integrated approach and should not be used as an excuse for delaying treatment at WWTP hotspots.
The UV/H2O2 technology tested at the two sites in this case study is extremely suitable, either in combination with anion exchange for EfOM removal as a permanent solution at WWTPs, or as a temporary solution for drinking water if the water quality is at risk. The technology has a small footprint, can be built in a modular fashion, and has a high removal efficiency for pharmaceutical compounds. Furthermore, it can be operated at reasonable cost.
5. Conclusions
This case study has indicated and confirmed that pharmaceuticals and their metabolites are present throughout the study area, originating from WWTP discharge. It has been shown that significant contributions from effluents can be observed in smaller tributaries. The WWTP effluent contributes to a large extent to the discharge and pollutant load. In our study it was observed that the top 10 of the highest concentrations of pharmaceuticals and metabolites determine 90% of the total load.
To tackle the challenge of pharmaceuticals in the water cycle, we envision a combined approach with a long-term approach to remove pharmaceutical compounds form WWTP effluent, with priority on hotspots. If the drinking water quality is at risk, a temporary treatment solution for the drinking water production with a small-footprint and modular flexible design can be considered. Based on our pilot plant results, both systems the use of UV oxidation could be a viable solution. On the WWTPs, this can be combined with EfOM removal to improve efficiency.
Supplementary Materials
The following are available online at https://www.mdpi.com/2073-4441/11/5/1034/s1, Figure S1: Sampling location Meuse at Eijsden, Figure S2: Sampling point Jeker at Maastricht, Figure S3: Sampling point Geul at Meerssen, Figure S4: Sampling point Geleenbeek at Oud-Roosteren, Figure S5: Sampling point Slijbeek, Figure S6: Sampling point at intake of Water Treatment Plant Heel, Lateraalkanaal, Figure S7: Discharge of the Meuse during 2011. The river showed an extreme low flow from May to early December. The black dots indicate the sampling dates for pharmaceuticals, Table S1: Concentrations of pharmaceuticals in the Lateraal Kanaal, measured at four different dates in 2011, Table S2: Concentrations of pharmaceuticals in the Slijbeek, measured at four different dates in 2011, Table S3: Concentrations of pharmaceuticals in the Geleenbeek, measured at four different dates in 2011, Table S4: Concentrations of pharmaceuticals in the Geul, measured at four different dates in 2011, Table S5: Concentrations of pharmaceuticals in the Jeker, measured at four different dates in 2011, Table S6: Concentrations of pharmaceuticals in the Meuse at Eijsden, measured at four different dates in 2011, Table S7: Concentrations of metabolites in the Lateraal Kanaal, measured at four different dates in 2011, Table S8: Concentrations of metabolites in the Slijbeek, measured at four different dates in 2011, Table S9: Concentrations of metabolites in the Geleenbeek, measured at four different dates in 2011, Table S10: Concentrations of metabolites in the Geul, measured at four different dates in 2011, Table S11: Concentrations of metabolites in the Jeker, measured at four different dates in 2011, Table S12: Concentrations of metabolites in the Meuse at Eijsden, measured at four different dates in 2011.
Author Contributions
Conceptualization, R.H.-C., T.t.L. and J.H.; Formal analysis, R.H.-C., T.t.L. and J.H.; Investigation, R.H.-C., T.t.L., H.H., H.T., A.d.M., P.v.D. and J.H.; Methodology, R.H.-C., T.t.L., H.H., H.T., A.d.M., P.v.D. and J.H.; Validation, R.H.-C.; Visualization, J.H.; Writing – original draft, R.H.-C.; Writing – review and editing, R.H.-C., T.t.L., H.H., H.T., P.v.D. and J.H.
Funding
This project has been co-financed with PPS-funding from the Topconsortia for Knowledge and Innovation (TKI’s) of the Ministry of Economic Affairs and Climate.
Acknowledgments
The authors would like to thank Waterleiding Maatschappij Limburg and Waterschapsbedrijf Limburg for providing data and their support for conducting the pilot plant research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Barbosa, M.O.; Moreira, N.F.F.; Ribeiro, A.R.; Pereira, M.F.R.; Silva, A.M.T. Occurrence and removal of organic micropollutants: An overview of the watch list of EU Decision 2015/495. Water Res. 2016, 94, 257–279. [Google Scholar] [CrossRef]
- Richardson, M.L.; Bowron, J.M. The fate of pharmaceutical chemicals in the aquatic environment. J. Pharm. Pharmacol. 1985, 37, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Daughton, C.G.; Ternes, T.A. Pharmaceuticals and personal care products in the environment: Agents of subtle change? Environ. Health Perspect. 1999, 107, 907–938. [Google Scholar] [CrossRef] [PubMed]
- Sui, Q.; Cao, X.; Lu, S.; Zhao, W.; Qiu, Z.; Yu, G. Occurrence, sources and fate of pharmaceuticals and personal care products in the groundwater: A review. Emerg. Contam. 2015, 1, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Van Der Aa, N.G.F.M.; Kommer, G.J.; Van Montfoort, J.E.; Versteegh, J.F.M. Demographic projections of future pharmaceutical consumption in the Netherlands. Water Sci. Technol. 2011, 63, 825–831. [Google Scholar] [CrossRef]
- Klein Tank, A.; Beersma, J.; Bessembinder, J.; van den Hurk, B.; Lenderink, G. KNMI ‘14; Klimaatscenario’s Voor Nederland, Leidraad Voor Professionals in Klimaatadaptatie; 2015 Revised Version; Royal Netherlands Meteorological Institute KNMI: De Bilt, The Netherlands, 2015. (In Dutch)
- Sjerps, R.M.A.; Ter Laak, T.L.; Zwolsman, G.J.J.G. Projected impact of climate change and chemical emissions on water quality of the European rivers Rhine and Meuse: A drinking water perspective. Sci. Total Environ. 2017, 601, 1682–1694. [Google Scholar] [CrossRef]
- Heberer, T. Occurrence, fate, and removal of pharmaceutical residues in the aquatic environment: A review of recent research data. Toxicol. Lett. 2002, 131, 5–17. [Google Scholar] [CrossRef]
- Kidd, K.A.; Blanchfield, P.J.; Mills, K.H.; Palace, V.P.; Evans, R.E.; Lazorchak, J.M.; Flick, R.W. Collapse of a fish population after exposure to a synthetic estrogen. Proc. Natl. Acad. Sci. USA 2007, 104, 8897–8901. [Google Scholar] [CrossRef] [Green Version]
- Crane, M.; Watts, C.; Boucard, T. Chronic aquatic environmental risks from exposure to human pharmaceuticals. Sci. Total Environ. 2006, 367, 23–41. [Google Scholar] [CrossRef]
- Santos, L.H.; Araújo, A.N.; Fachini, A.; Pena, A.; Delerue-Matos, C.; Montenegro, M.C.B.S.M. Ecotoxicological aspects related to the presence of pharmaceuticals in the aquatic environment. J. Hazard. Mater. 2010, 175, 45–95. [Google Scholar] [CrossRef] [Green Version]
- Brodin, T.; Piovano, S.; Fick, J.; Klaminder, J.; Heynen, M.; Jonsson, M. Ecological effects of pharmaceuticals in aquatic systems—Impacts through behavioural alterations. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Commission Implementing Decision (EU) 2015/495 of 20 March 2015 Establishing a Watch List of Substances for Union-Wide Monitoring in the Field of Water Policy Pursuant to Directive 2008/105/EC of the European Parliament and of the Council. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32015D0495&from=EN (accessed on 22 October 2018).
- Carvalho, R.N.; Ceriani, L.; Ippolito, A.; Lettieri, T. Development of the first Watch List under the Environmental Quality Standards Directive; EC Joint Research Centre: Ispra, Italy, 2015. [Google Scholar]
- European Commission. Proposal for a Directive of the European Parliament and of the Council on the Quality of Water Intended for Human Consumption (Recast). Available online: http://eur-lex.europa.eu/resource.html?uri=cellar:8c5065b2-074f-11e8-b8f5-01aa75ed71a1.0016.02/DOC_1&format=PDF (accessed on 22 October 2018).
- Van der Grinten, E.; van der Maaden, T.; van Vlaardingen, P.L.A.; Venhuis, B.J.; Moermond, C.T.A. Milieuafwegingen in de Geneesmiddelvoorziening; Rijksinstituut voor Volksgezondheid en Milieu; Ministerie van Volksgezondheid, Welzijn en Sport: Bilthoven, The Netherlands, 2017. (In Dutch)
- Waterschap Drents Overijsselse Delta. Evaluatie van het Project Milieubewust Medicijnen Voorschrijven Door Huisartsen in Meppel; Waterschap Drents Overijsselse Delta: Meppel, The Netherlands, 2017. (In Dutch) [Google Scholar]
- Mulder, M.; Antakyali, D.; Ante, S. Verwijdering van Microverontreinigingen uit Effluenten van RWZI’s: Een Vertaling van Kennis en Ervaring uit Duitsland en Zwitserland.; Stichting Toegepast Onderzoek Waterbeheer (STOWA): Amersfoort, The Netherlands, 2015. (In Dutch) [Google Scholar]
- Varanasi, L.; Coscarelli, E.; Khaksari, M.; Mazzoleni, L.R.; Minakata, D. Transformations of dissolved organic matter induced by UV photolysis, Hydroxyl radicals, chlorine radicals, and sulfate radicals in aqueous-phase UV-Based advanced oxidation processes. Water Res. 2018, 135, 22–30. [Google Scholar] [CrossRef]
- Nihemaiti, M.; Miklos, D.B.; Hübner, U.; Linden, K.G.; Drewes, J.E.; Croué, J.P. Removal of trace organic chemicals in wastewater effluent by UV/H2O2 and UV/PDS. Water Res. 2018, 145, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Miklos, D.B.; Hartl, R.; Michel, P.; Linden, K.G.; Drewes, J.E.; Hübner, U. UV/H2O2 process stability and pilot-scale validation for trace organic chemical removal from wastewater treatment plant effluents. Water Res. 2018, 136, 169–179. [Google Scholar] [CrossRef]
- Miklos, D.B.; Remy, C.; Jekel, M.; Linden, K.G.; Drewes, J.E.; Hübner, U. Evaluation of advanced oxidation processes for water and wastewater treatment—A critical review. Water Res. 2018, 139, 118–131. [Google Scholar] [CrossRef]
- Miklos, D.B.; Wang, W.L.; Linden, K.G.; Drewes, J.E.; Hübner, U. Comparison of UV-AOPs (UV/H2O2, UV/PDS and UV/Chlorine) for TOrC removal from municipal wastewater effluent and optical surrogate model evaluation. Chem. Eng. J. 2019, 362, 537–547. [Google Scholar] [CrossRef]
- Guo, K.; Wu, Z.; Yan, S.; Yao, B.; Song, W.; Hua, Z.; Zhang, X.; Kong, X.; Li, X.; Fang, J. Comparison of the UV/chlorine and UV/H2O2 processes in the degradation of PPCPs in simulated drinking water and wastewater: Kinetics, radical mechanism and energy requirements. Water Res. 2018, 147, 184–194. [Google Scholar] [CrossRef]
- Ter Laak, T.; Tolkamp, H.; Hofman, J. Geneesmiddelen in de Watercyclus in Limburg; KWR Watercycle Research Institute: Nieuwegein, The Netherlands, 2013. (In Dutch) [Google Scholar]
- Huber, S.A.; Balz, A.; Abert, M.; Pronk, W. Characterisation of aquatic humic and non-humic matter with size-exclusion chromatography—Organic carbon detection—Organic nitrogen detection (LC-OCD-OND). Water Res. 2011, 45, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Hofman-Caris, C.H.M.; Harmsen, D.J.H.; Van Remmen, A.M.; Knol, A.H.; Van Pol, W.L.C.; Wols, B.A. Optimization of UV/H2O2 processes for the removal of organic micropollutants from drinking water: Effect of reactor geometry and water pretreatment on EEO values. Water Sci. Technol. 2017, 17, 508–518. [Google Scholar] [CrossRef]
- Wols, B.A.; Hofman-Caris, C.H.M.; Harmsen, D.J.H.; Beerendonk, E.F. Degradation of 40 selected pharmaceuticals by UV/H2O2. Water Res. 2013, 47, 5876–5888. [Google Scholar] [CrossRef]
- Hofman-Caris, C.H.M.; Siegers, W.G.; van de Merlen, K.; de Man, A.W.A.; Hofman, J.A.M.H. Removal of pharmaceuticals from WWTP effluent: Removal of EfOM followed by advanced oxidation. Chem. Eng. J. 2017, 327, 514–521. [Google Scholar] [CrossRef]
- Wols, B.A.; Harmsen, D.J.H.; van Remmen, T.; Beerendonk, E.F.; Hofman-Caris, C.H.M. Design aspects of UV/H2O2 reactors. Chem. Eng. Sci. 2015, 137, 712–721. [Google Scholar] [CrossRef]
- Vergouwen, A.A.; Pieters, B.J.; Kools, S. ZORG Inventarisatie van Emissie van Geneesmiddelen uit Zorginstellingen; Part C; Stichting Toegepast Onderzoek Waterbeheer (STOWA): Amersfoort, The Netherlands, 2011. (In Dutch) [Google Scholar]
- Niemuth, N.J.; Jordan, R.; Crago, J.; Blanksma, C.; Johnson, R.; Klaper, R.D. Metformin exposure at environmentally relevant concentrations causes potential endocrine disruption in adult male fish. Environ. Toxicol. Chem. 2015, 34, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Niemuth, N.J.; Klaper, R.D. Emerging wastewater contaminant metformin causes intersex and reduced fecundity in fish. Chemosphere 2015, 135, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Société Publique de Gestion de l’Eau. Plan Dássainissement par Sous-Bassin Hydrographique (PASH); Société Publique de Gestion de l’Eau: Verviers, Belgium, 2005. (In French) [Google Scholar]
- Ter Laak, T.L.; Kooij, P.J.F.; Tolkamp, H.; Hofman, J. Different compositions of pharmaceuticals in Dutch and Belgian rivers explained by consumption patterns and treatment efficiency. Environ. Sci. Pollut. Res. 2014, 21, 12843–12855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourgin, M.; Beck, B.; Boehler, M.; Borowska, E.; Fleiner, J.; Salhi, E.; Teichler, R.; von Gunten, U.; Siegrist, H.; McArdell, C.S. Evaluation of a full-scale wastewater treatment plant upgraded with ozonation and biological post-treatments: Abatement of micropollutants, formation of transformation products and oxidation by-products. Water Res. 2018, 129, 486–498. [Google Scholar] [CrossRef]
- Coppens, L.J.C.; van Gils, J.A.G.; ter Laak, T.L.; Raterman, B.W.; van Wezel, A.P. Towards spatially smart abatement of human pharmaceuticals in surface waters: Defining impact of sewage treatment plants on susceptible functions. Water Res. 2015, 81, 356–365. [Google Scholar] [CrossRef]
- Kümmerer, K. Chapter 7 Benign by design. In Green and Sustainable Medicinal Chemistry: Methods, Tools and Strategies for the 21st Century Pharmaceutical Industry; Somerton, L., Sneddon, H.F., Jones, L.C., Clark, J.H., Eds.; RSC Green Chemistry: Cambridge, UK, 2016; pp. 73–81. [Google Scholar] [CrossRef]
Figure 1.
(a): Wastewater treatment plants (WWTPs) in The Netherlands (red dots) and WWTPs sampled for effluent characterization (green-red dots, indicated A to F); (b): Sample locations in surface water bodies (blue dots, indicated 1 to 6) in the southern part of the province of Limburg.
Figure 1.
(a): Wastewater treatment plants (WWTPs) in The Netherlands (red dots) and WWTPs sampled for effluent characterization (green-red dots, indicated A to F); (b): Sample locations in surface water bodies (blue dots, indicated 1 to 6) in the southern part of the province of Limburg.

Figure 2.
Concentrations of pharmaceuticals (left two graphs) and metabolites (right graph) in WWTP effluents in The Netherlands. The concentrations of metformin and its metabolite guanylurea are present in significantly higher concentrations, and therefore shown separately in the lower right graph.
Figure 2.
Concentrations of pharmaceuticals (left two graphs) and metabolites (right graph) in WWTP effluents in The Netherlands. The concentrations of metformin and its metabolite guanylurea are present in significantly higher concentrations, and therefore shown separately in the lower right graph.

Figure 3.
Average concentrations (n = 4) of pharmaceuticals and their metabolites detected in the River Meuse and its tributaries.
Figure 3.
Average concentrations (n = 4) of pharmaceuticals and their metabolites detected in the River Meuse and its tributaries.

Figure 4.
Contribution of several sources to the pharmaceutical and metabolite concentration at the intake of drinking water production site Heel. The dark shaded bars are based on load predictions from the actual measurements of concentrations and discharges in November and December 2011. The lighter shaded bars are generalized load predictions for low (comparable to November), median (comparable to December) and extremely high discharge.
Figure 4.
Contribution of several sources to the pharmaceutical and metabolite concentration at the intake of drinking water production site Heel. The dark shaded bars are based on load predictions from the actual measurements of concentrations and discharges in November and December 2011. The lighter shaded bars are generalized load predictions for low (comparable to November), median (comparable to December) and extremely high discharge.

Figure 5.
Removal of pharmaceuticals (left graph) and metabolites (right graph) in the effluent of WWTP Panheel, by applying ultraviolet (UV)/H2O2 at a UV dose of 150 and 300 mJ/cm2.
Figure 5.
Removal of pharmaceuticals (left graph) and metabolites (right graph) in the effluent of WWTP Panheel, by applying ultraviolet (UV)/H2O2 at a UV dose of 150 and 300 mJ/cm2.

Figure 6.
Removal of pharmaceuticals (left graph) and metabolites (right graph) at drinking water production site Heel, applying a UV dose of 365 mJ/cm2 and a H2O2 concentration of 10 mg/L.
Figure 6.
Removal of pharmaceuticals (left graph) and metabolites (right graph) at drinking water production site Heel, applying a UV dose of 365 mJ/cm2 and a H2O2 concentration of 10 mg/L.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Most common pharmaceuticals and metabolites detected in the River Meuse and its tributaries in The Netherlands, expressed as the average contribution (%) to the total load of pharmaceuticals and transformation products analyzed.
Table 1.
Most common pharmaceuticals and metabolites detected in the River Meuse and its tributaries in The Netherlands, expressed as the average contribution (%) to the total load of pharmaceuticals and transformation products analyzed.
| Meuse | Meuse | Geul | Geleenbeek | Slijbeek | Jeker | |
|---|---|---|---|---|---|---|
| ‘Low’ | ‘High’ | |||||
| Discharge (m3/s) | 14 1 | 253 2 | 2.8 3 | 2.1 3 | 0.1 4 | 1.7 3 |
| Near minimum | Above nominal | Nominal | Nominal | Estimated | Nominal | |
| Proportion of WWTP effluent to discharge (%) | No data available | No data available | 15 | 38 | 51 | Unknow; untreated discharges |
| Total pharmaceuticals load (kg/day) | 10 | 106 | 1.4 | 4.9 | 0.1 | 2.2 |
| guanylurea | 25% | 12% | 40% | 60% | 68% | 20% |
| metformine | 47% | 49% | 22% | 13% | 6% | 39% |
| 10,11-trans-diol-carbamazepine | 2% | 2% | 3% | 4% | 5% | 2% |
| metoprolol | 0% | 0% | 3% | 3% | 3% | 0% |
| sotalol | 2% | 2% | 4% | 3% | 3% | 3% |
| hydroxy ibuprofen | 6% | 10% | 9% | 3% | 2% | 9% |
| furosemide | 0% | 0% | 1% | 2% | 1% | 1% |
| tramadol | 2% | 2% | 2% | 2% | 1% | 4% |
| atenolol | 1% | 1% | 0% | 1% | 1% | 1% |
| carbamazepine | 1% | 1% | 1% | 1% | 2% | 1% |
| diclofenac | 1% | 1% | 2% | 1% | 0% | 1% |
| Other 26 compounds | 13% | 19% | 13% | 7% | 8% | 19% |
1 November 2011; 2 December 2011; 3 Measurements every 15 min, 1-1-2008 to 21-12-2011; 4 Estimated by the Water Authority ‘Peel en Maasvallei’.
Table 2.
Potential abatement options to improve quality of surface waters and the source water for drinking water treatment at the production site Heel.
Table 2.
Potential abatement options to improve quality of surface waters and the source water for drinking water treatment at the production site Heel.
| Abatement Option | Effect on Drinking Water | Effect on Surface Water | Total Additional Costs 1 | Advantages | Disadvantages |
|---|---|---|---|---|---|
| Prevent and reduce pharmaceutical emission at source (toilets) | Effective | Effective | unknown | Protects aquatic environment | Difficult to realize; long-term effects |
| Different layout of water system; diverting WWTP effluent downstream of the drinking water intake | Effective | Not effective | low | Quick solution | Emergency measure |
| Extension of individual WWTPs | Not effective unless realized on multiple locations | Effective for small surface waters | 8–15 M€/year | Local improvement of surface water quality | Only effective for drinking water on long-term and at large-scale application |
| Extension of WWTPs on a large, international scale | Effective | Effective | 8–15 M€/year in The Netherlands | Strong improvement of surface water quality | Long-term realization |
| Extension drinking water treatment | Effective | Not effective | 4–8 M€/year | Short-term realization | No improvement of surface water quality |
1 Costs are calculated based on the cost standard and related calculator, developed by the Dutch water sector. See www.kostenstandaard.nl.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hofman-Caris, R.; ter Laak, T.; Huiting, H.; Tolkamp, H.; de Man, A.; van Diepenbeek, P.; Hofman, J. Origin, Fate and Control of Pharmaceuticals in the Urban Water Cycle: A Case Study. Water 2019, 11, 1034. https://doi.org/10.3390/w11051034
AMA Style
Hofman-Caris R, ter Laak T, Huiting H, Tolkamp H, de Man A, van Diepenbeek P, Hofman J. Origin, Fate and Control of Pharmaceuticals in the Urban Water Cycle: A Case Study. Water. 2019; 11(5):1034. https://doi.org/10.3390/w11051034
Chicago/Turabian StyleHofman-Caris, Roberta, Thomas ter Laak, Hans Huiting, Harry Tolkamp, Ad de Man, Peter van Diepenbeek, and Jan Hofman. 2019. "Origin, Fate and Control of Pharmaceuticals in the Urban Water Cycle: A Case Study" Water 11, no. 5: 1034. https://doi.org/10.3390/w11051034
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.